

Does HIV Exploit the Inflammatory Milieu of the Male Genital Tract for Successful Infection?
- PMID: 27446076
- PMCID: PMC4919362
- DOI: 10.3389/fimmu.2016.00245
Does HIV Exploit the Inflammatory Milieu of the Male Genital Tract for Successful Infection?
Abstract
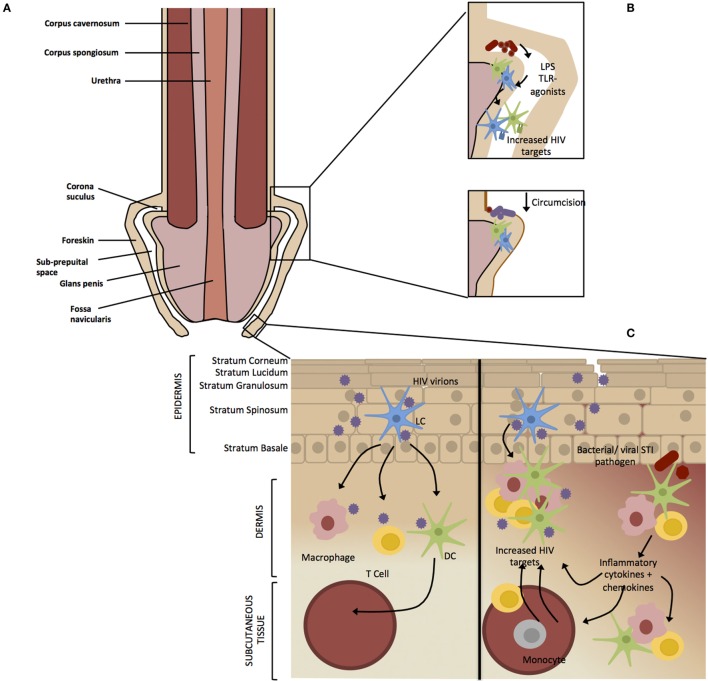
In many parts of the World, medical male circumcision (MMC) is used as standard prevention of care against HIV infection. This is based on seminal reports made over 10 years ago that removal of the foreskin provides up to 60% protection against HIV infection in males and seems currently the best antiretroviral-free prevention strategy yet against the global epidemic. We explore the potential mechanisms by which MMC protects against HIV-1 acquisition and that one of the oldest, albeit re-invented, rituals of removing a foreskin underscores the exploitative nature of HIV on the anatomy and tissue of the uncircumcised penis. Furthermore, foreskin removal also reveals how males acquire HIV, and in reality, the underlying mechanisms of MMC are not known. We argue that the normal sequelae of inflammation in the male genital tract (MGT) for protection from sexually transmitted infections (STI)-induced pathology represents a perfect immune and microbial ecosystem for HIV acquisition. The accumulation of HIV-1 target cells in foreskin tissue and within the urethra in response to STIs, both during and after resolution of infection, suggests that acquisition of HIV-1, through sexual contact, makes use of the natural immune milieu of the MGT. Understanding immunity in the MGT, the movement of HIV-1 target cells to the urethra and foreskin tissue upon encounter with microbial signals would provide more insight into viral acquisition and lay the foundation for further prevention strategies in males that would be critical to curb the epidemic in all sexual partners at risk of infection. The global female-centric focus of HIV-1 transmission and acquisition research has tended to leave gaps in our knowledge of what determines HIV-1 acquisition in men and such understanding would provide a more balanced and complete view of viral acquisition.
Keywords: HIV-1; acquisition; exploitation; inflammation; medical male circumcision; risk factors; sexually transmitted infections.
Figures
References
-
- Unaids. UNAIDS: The Gap Report 26. Geneva: Joint United Nations Programme on HIV/AIDS; (2014).
-
- UNAIDS. Global AIDS response progress reporting 2014: Construction of Core Indicators for Monitoring the 2011 UN Political Declaration on HIV/AIDS. Geneva: Joint United Nations Programme on HIV/AIDS; (2014).
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical