

Recurrence patterns in patients with high-grade glioma following temozolomide-based chemoradiotherapy
- PMID: 27446566
- PMCID: PMC4950878
- DOI: 10.3892/mco.2016.936
Recurrence patterns in patients with high-grade glioma following temozolomide-based chemoradiotherapy
Abstract
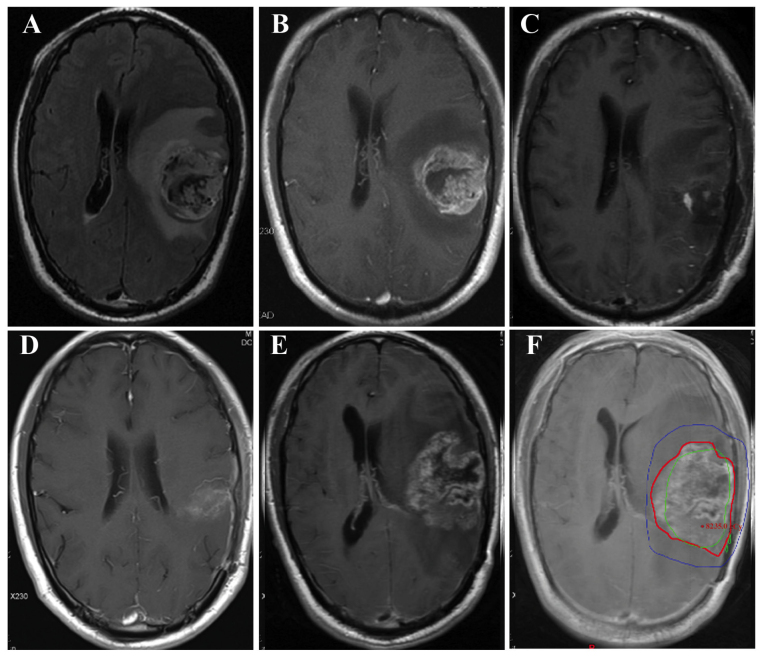
There is currently no consensus regarding the optimal radiation volume for high-grade glioma (HGG). The brain volume irradiated is associated with the extent of radiation neurotoxicity. When reducing the treatment volume, the risk of geographic tumor miss should be considered. In such cases, the recurrence patterns and, particularly, the rate of marginal tumor recurrence, are important indices for determining the optimal radiation volume. In the present study, a smaller-target delineation protocol with limited margins was adopted. The postoperative enhancing tumor and resection cavity were defined as gross tumor volume (GTV); 1 and 2 cm were added to the GTV to create clinical target volume (CTV1 and CTV2), which received 60 and 54 Gy, respectively. At a median follow-up of 14 months, 54 HGG patients developed tumor recurrence. The median overall and progression-free survival were 14 and 10.5 months, respectively. A total of 34 patients developed central recurrence, 8 presented with in-field recurrence, 2 developed marginal recurrence, 2 had distant recurrence and 11 patients developed cerebrospinal fluid dissemination, 2 of whom developed central recurrence, with 1 patient simultaneously developing marginal recurrence. Local recurrence (central and in-field) was found to be the main recurrence pattern. As the rate of marginal recurrence was low (<5%), it appears that the smaller irradiated volume in the present study was appropriate. However, clinical trials investigating limited irradiation volume are required to validate our findings.
Keywords: chemoradiotherapy; high-grade glioma; irradiated volume; recurrence patterns.
Figures
References
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. doi: 10.1016/S1470-2045(09)70025-7. - DOI - PubMed
-
- Chang C, Horton J, Schoenfeld D, Salazer O, Perez-Tamayo R, Kramer S, Weinstein A, Nelson J, Tsukada Y. Comparison of postoperative radiotherapy and combined postoperative radiotherapy and chemotherapy in the multidisciplinary management of malignant gliomas. A joint Radiation Therapy Oncology Group and Eastern Cooperative Oncology Group study. Cancer. 1983;52:997–1007. doi: 10.1002/1097-0142(19830915)52:6<997::AID-CNCR2820520612>3.0.CO;2-2. - DOI - PubMed
-
- Nelson DF, Curran WJ, Jr, Scott C, Nelson JS, Weinstein AS, Ahmad K, Constine LS, Murray K, Powlis WD, Mohiuddin M, et al. Hyperfractionated radiation therapy and bis-chlorethyl nitrosourea in the treatment of malignant glioma - possible advantage observed at 72.0 Gy in 1.2 Gy B.I.D. fractions: Report of the Radiation Therapy Oncology Group protocol 8302. Int J Radiat Oncol Biol Phys. 1993;25:193–207. doi: 10.1016/0360-3016(93)90340-2. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials