

Dose response of task-specific upper limb training in people at least 6 months poststroke: A phase II, single-blind, randomized, controlled trial
- PMID: 27447365
- PMCID: PMC5016233
- DOI: 10.1002/ana.24734
Dose response of task-specific upper limb training in people at least 6 months poststroke: A phase II, single-blind, randomized, controlled trial
Abstract
Objective: The objectives of this work were to (1) determine whether higher doses of motor therapy in chronic poststroke hemiparesis result in better outcomes, compared to lower doses, and (2) evaluate potential modifiers of the dose-response relationship.
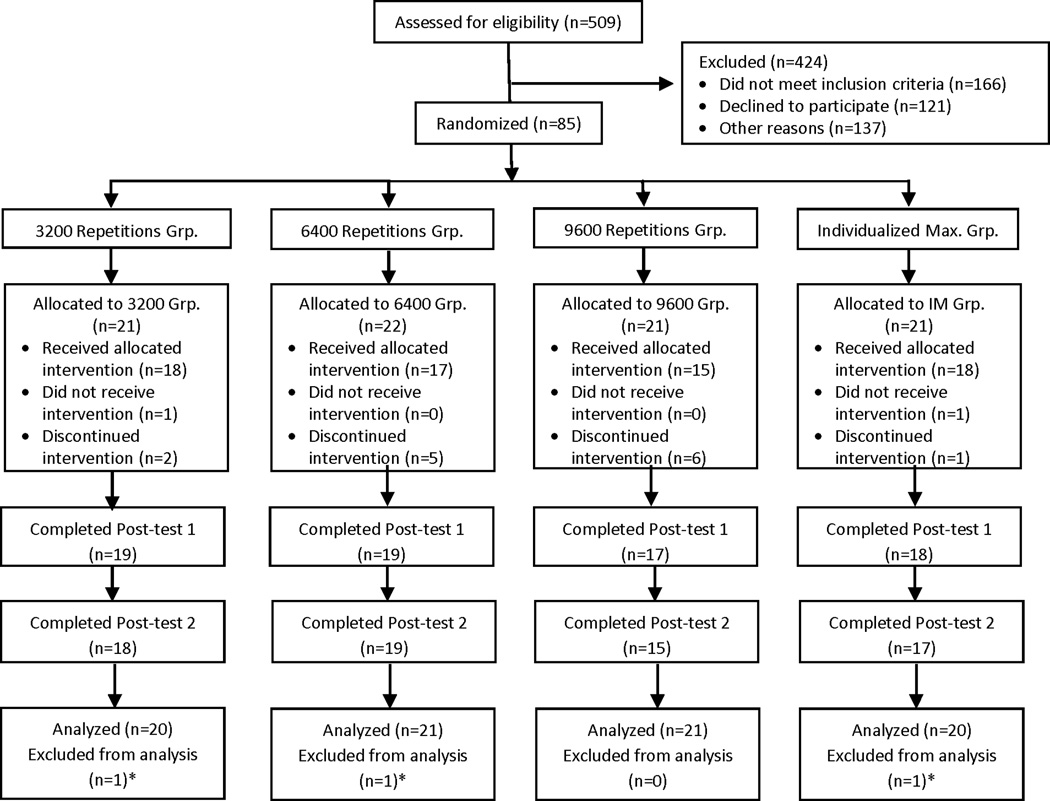
Methods: Eighty-five adults with upper extremity paresis ≥6 months poststroke were randomized to one of four dose groups in this single-blind, parallel, randomized, control trial. The dosing parameter manipulated was amount of task-specific training, as indexed by the number of task repetitions. Groups received 3,200, 6,400, 9,600, or individualized maximum (IM) repetitions, during 1-hour sessions, 4 days/week for 8 weeks. The intervention was an individualized, progressive, task-specific upper-limb training program designed to improve upper-limb functional motor capacity. The primary outcome was the slope of the Action Research Arm Test (ARAT) during the intervention. Effects of dose and potential modifiers of the dose-response relationship were evaluated with hierarchical linear models.
Results: ARAT scores for the 3,200, 9,600, and IM groups improved over time as indicated by slopes (ΔARAT/week, mean ± standard errors) of 0.40 ± 0.15, 0.31 ± 0.16, and 0.66 ± 0.14, respectively (p < 0.05). The slope of the 6,400 group was smaller (-0.05 ± 0.15) and significantly different from the 3,200 and IM groups (p < 0.001). Initial motor capacity, neglect, and other tested characteristics did not modify the dose-response relationship.
Interpretation: Overall, treatment effects were small. There was no evidence of a dose-response effect of task-specific training on functional capacity in people with long-standing upper-limb paresis poststroke. Ann Neurol 2016;80:342-354.
© 2016 American Neurological Association.
Conflict of interest statement
There are no potential conflicts of interest between the authors and any commercial sponsors.
Figures

Comment in
-
What's the perfect dose for practice to make perfect?Ann Neurol. 2016 Sep;80(3):339-41. doi: 10.1002/ana.24735. Epub 2016 Aug 13. Ann Neurol. 2016. PMID: 27447540 No abstract available.
References
-
- Ross LF, Harvey LA, Lannin NA. Do people with acquired brain impairment benefit from additional therapy specifically directed at the hand? A randomized controlled trial. Clinical rehabilitation. 2009;23:492–503. - PubMed
-
- Hsu SS, Hu MH, Wang YH, Yip PK, Chiu JW, Hsieh CL. Dose-response relation between neuromuscular electrical stimulation and upper-extremity function in patients with stroke. Stroke; a journal of cerebral circulation. 2010;41:821–824. - PubMed
-
- Harris JE, Eng JJ, Miller WC, Dawson AS. A self-administered graded repetitive arm supplementary program (grasp) improves arm function during inpatient stroke rehabilitation: A multi-site randomized controlled trial. Stroke; a journal of cerebral circulation. 2009;40:2123–2128. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
