

Treatment for Multiple Acute Cardiopulmonary Conditions in Older Adults Hospitalized with Pneumonia, Chronic Obstructive Pulmonary Disease, or Heart Failure
- PMID: 27448329
- PMCID: PMC4988873
- DOI: 10.1111/jgs.14303
Treatment for Multiple Acute Cardiopulmonary Conditions in Older Adults Hospitalized with Pneumonia, Chronic Obstructive Pulmonary Disease, or Heart Failure
Abstract
Objectives: To determine how often hospitalized older adults principally diagnosed with pneumonia, chronic obstructive pulmonary disease (COPD), or heart failure (HF) are concurrently treated for two or more of these acute cardiopulmonary conditions.
Design: Retrospective cohort study.
Setting: 368 U.S. hospitals in the Premier research database.
Participants: Individuals aged 65 and older principally hospitalized with pneumonia, COPD, or HF in 2009 or 2010.
Measurements: Proportion of diagnosed episodes of pneumonia, COPD, or HF concurrently treated for two or more of these acute cardiopulmonary conditions during the first 2 hospital days.
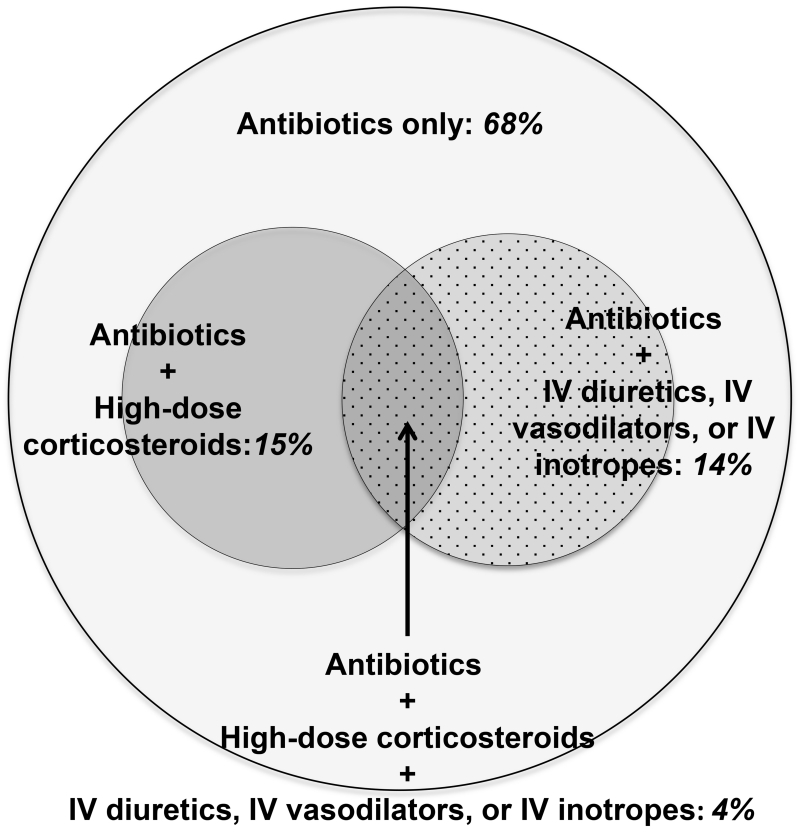
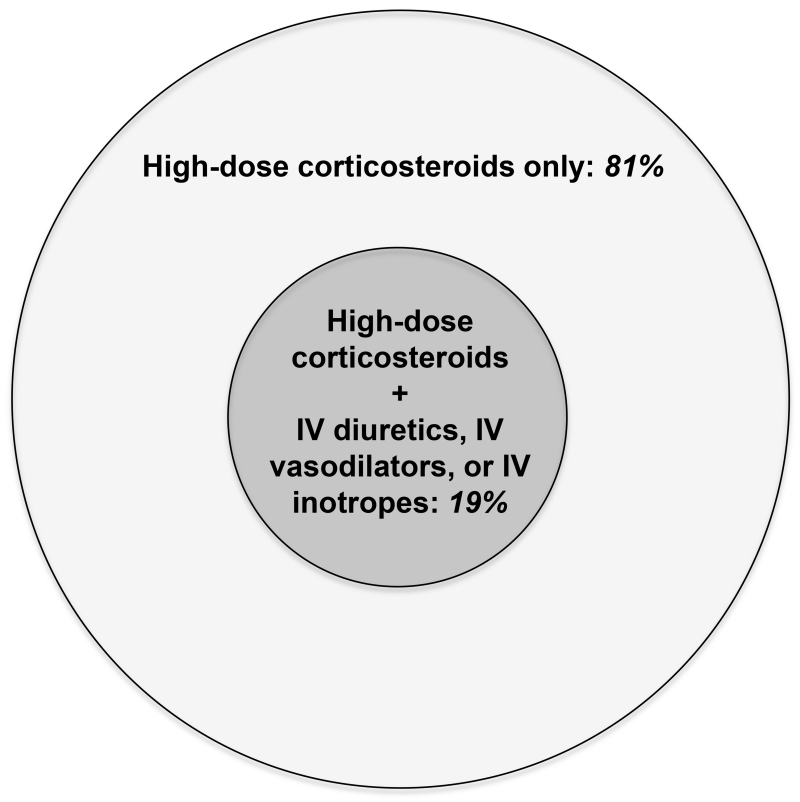
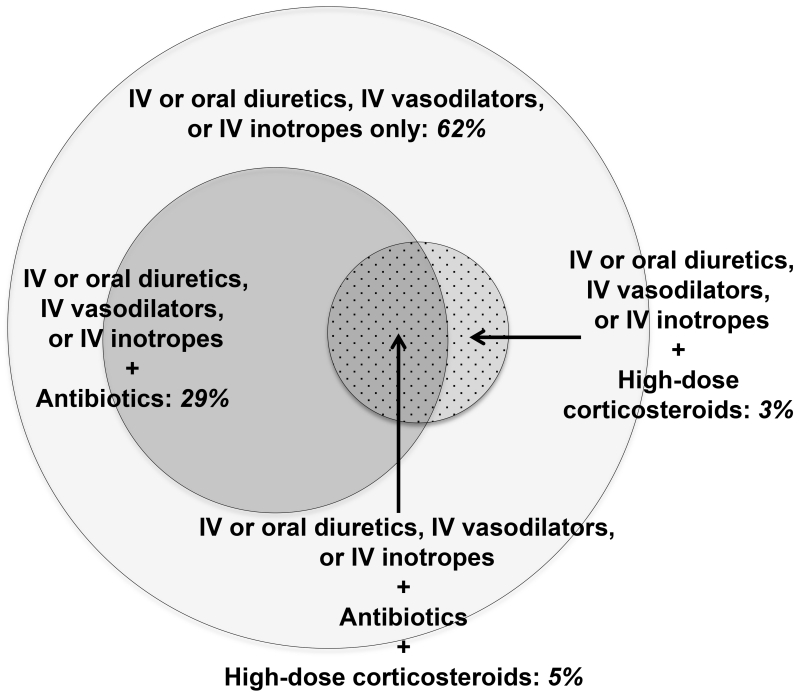
Results: Of 91,709 diagnosed pneumonia hospitalizations, 32% received treatment for two or more acute cardiopulmonary conditions (18% for HF, 18% for COPD, 4% for both). Of 41,052 diagnosed COPD hospitalizations, 19% received treatment for two or more acute cardiopulmonary conditions (all of which involved additional HF treatment). Of 118,061 diagnosed HF hospitalizations, 38% received treatment for two or more acute cardiopulmonary conditions (34% for pneumonia, 9% for COPD, 5% for both).
Conclusion: Hospitalized older adults diagnosed with pneumonia, COPD, or HF are frequently treated for two or more acute cardiopulmonary conditions, suggesting that clinical syndromes often fall between traditional diagnostic categories. Research is needed to evaluate the risks and benefits of real-world treatment for the many older adults whose presentations elicit diagnostic uncertainty or concern about coexisting acute conditions.
Keywords: cardiovascular disease; comorbidity; hospital medicine; pharmacoepidemiology; pulmonary diseases.
© 2016, Copyright the Authors Journal compilation © 2016, The American Geriatrics Society.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) [Accessed February 27, 2015];Global strategy for the diagnosis, management and prevention of COPD. 2011 Available at: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2011_Feb21.pdf.
-
- Hunt SA, Abraham WT, Chin MH, et al. 2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: Developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119:e391–479. - PubMed
-
- Donowitz GR. Acute pneumonia. In: Mandell GL, Bennett JE, Dolin R, editors. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. 7th ed. Churchill Livingstone Elsevier; Philadelphia, PA: 2010. pp. 891–916.
-
- Shapiro SD, Reilly JJ, Rennard SI. Chronic bronchitis and emphysema. In: Mason RJ, Broaddus VC, Martin TR, et al., editors. Murray and Nadel’s Textbook of Respiratory Medicine. 5th ed. Saunders Elsevier; Philadelphia, PA: 2010. pp. 919–967.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
