

A nomogram composed of clinicopathologic features and preoperative serum tumor markers to predict lymph node metastasis in early gastric cancer patients
- PMID: 27449100
- PMCID: PMC5312336
- DOI: 10.18632/oncotarget.10732
A nomogram composed of clinicopathologic features and preoperative serum tumor markers to predict lymph node metastasis in early gastric cancer patients
Abstract
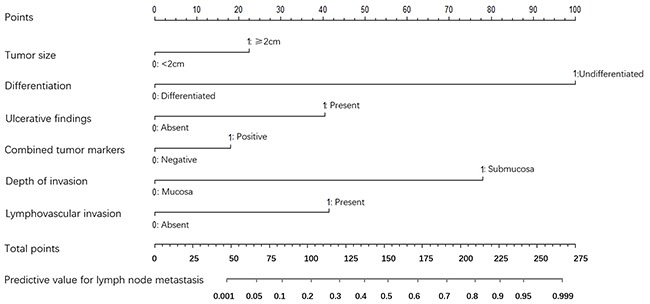
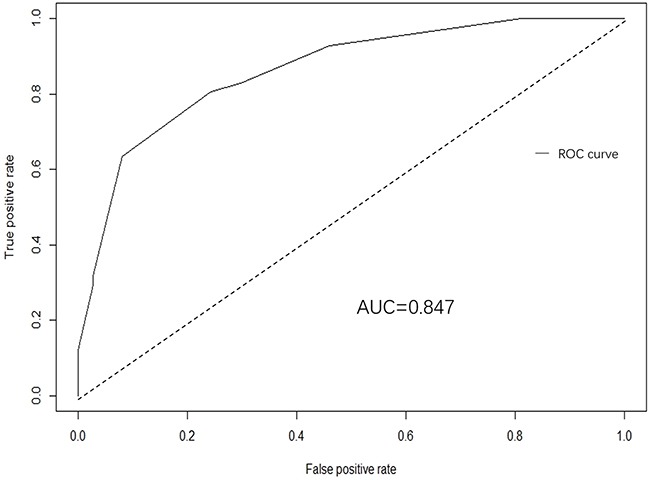
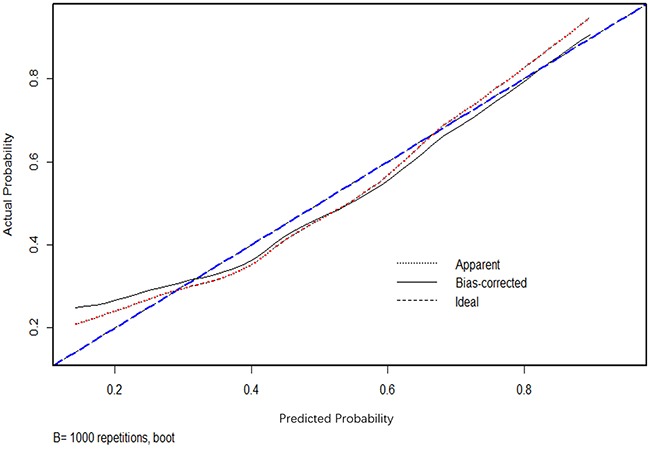
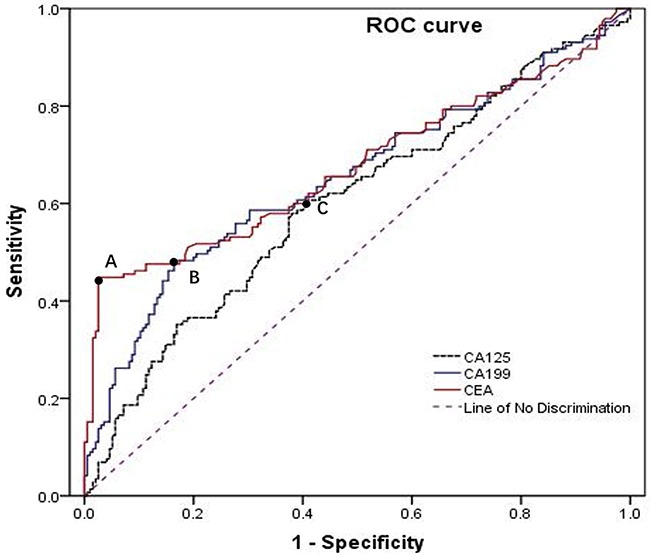
Predicting lymph node metastasis (LNM) accurately is of great importance to formulate optimal treatment strategies preoperatively for patients with early gastric cancer (EGC). This study aimed to explore risk factors that predict the presence of LNM in EGC. A total of 697 patients underwent gastrectomy enrolled in this study, were divided into training and validation set, and the relationship between LNM and other clinicopathologic features, preoperative serum combined tumor markers (CEA, CA19-9, CA125) were evaluated. Risk factors for LNM were identified using logistic regression analysis, and a nomogram was created by R program to predict the possibility of LNM in training set, while receiver operating characteristic (ROC) analysis was applied to assess the predictive value of the nomogram model in validation set. Consequently, LNM was significantly associated with tumor size, macroscopic type, differentiation type, ulcerative findings, lymphovascular invasion, depth of invasion and combined tumor marker. In multivariate logistic regression analysis, factors including of tumor size, differentiation type, ulcerative findings, lymphovascular invasion, depth of invasion and combined tumor marker were demonstrated to be independent risk factors for LNM. Moreover, a predictive nomogram with these independent factors for LNM in EGC patients was constructed, and ROC curve demonstrated a good discrimination ability with the AUC of 0.847 (95% CI: 0.789-0.923), which was significantly larger than those produced in previous studies. Therefore, including of these tumor markers which could be convenient and feasible to obtain from the serum preoperatively, the nomogram could effectively predict the incidence of LNM for EGC patients.
Keywords: early gastric cancer; lymph node metastasis; nomogram; prediction; tumor markers.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
[A nomogram for predicting lymph node metastasis in early gastric cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Jan 25;25(1):40-47. doi: 10.3760/cma.j.cn441530-20210208-00059. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35067033 Chinese.
-
The significance of preoperative serum carcinoembryonic antigen levels in the prediction of lymph node metastasis and prognosis in locally advanced gastric cancer: a retrospective analysis.BMC Gastroenterol. 2020 Apr 10;20(1):100. doi: 10.1186/s12876-020-01255-6. BMC Gastroenterol. 2020. PMID: 32276616 Free PMC article.
-
Risk factors of lymph node metastasis or lymphovascular invasion for early gastric cancer: a practical and effective predictive model based on international multicenter data.BMC Cancer. 2019 Nov 6;19(1):1048. doi: 10.1186/s12885-019-6147-6. BMC Cancer. 2019. PMID: 31694573 Free PMC article.
-
External validation of CEA and CA125 prediction model for lymph node metastasis in endometrial cancer: A multi-institute cohort study.Cancer Biomark. 2025 Mar;42(3):18758592241306265. doi: 10.1177/18758592241306265. Epub 2025 Apr 4. Cancer Biomark. 2025. PMID: 40183305
-
[Artificial intelligence for lymph node metastasis prediction in gastric cancer: research progress].Zhonghua Wei Chang Wai Ke Za Zhi. 2025 Jan 25;28(1):95-102. doi: 10.3760/cma.j.cn441530-20240510-00172. Zhonghua Wei Chang Wai Ke Za Zhi. 2025. PMID: 39971559 Review. Chinese.
Cited by
-
Meta-analysis of the prognostic value of long non-coding RNA AFAP1-AS1 for cancer patients in China.Oncotarget. 2017 Dec 21;9(8):8100-8110. doi: 10.18632/oncotarget.23568. eCollection 2018 Jan 30. Oncotarget. 2017. PMID: 29487718 Free PMC article.
-
Establishment of Decision Rules and Risk Assessment Model for Preoperative Prediction of Lymph Node Metastasis in Gastric Cancer.Front Oncol. 2020 Sep 2;10:1638. doi: 10.3389/fonc.2020.01638. eCollection 2020. Front Oncol. 2020. PMID: 32984033 Free PMC article.
-
A population-based study: how to identify high-risk T1 gastric cancer patients?Am J Cancer Res. 2021 Apr 15;11(4):1463-1479. eCollection 2021. Am J Cancer Res. 2021. PMID: 33948368 Free PMC article.
-
Construction and external validation of a nomogram that predicts lymph node metastasis in early gastric cancer patients using preoperative parameters.Chin J Cancer Res. 2018 Dec;30(6):623-632. doi: 10.21147/j.issn.1000-9604.2018.06.07. Chin J Cancer Res. 2018. PMID: 30700931 Free PMC article.
-
Prognostic and clinical significance of long non-coding RNA HNF1A-AS1 in solid cancers: A systematic review and meta-analysis.Medicine (Baltimore). 2019 Dec;98(49):e18264. doi: 10.1097/MD.0000000000018264. Medicine (Baltimore). 2019. PMID: 31804362 Free PMC article.
References
-
- Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–132. - PubMed
-
- Saragoni L, Morgagni P, Gardini A, Marfisi C, Vittimberga G, Garcea D, Scarpi E. Early gastric cancer: diagnosis, staging, and clinical impact. Evaluation of 530 patients. New elements for an updated definition and classification. Gastric Cancer. 2013;16:549–554. - PubMed
-
- Yanai H, Matsumoto Y, Harada T, Nishiaki M, Tokiyama H, Shigemitsu T, Tada M, Okita K. Endoscopic ultrasonography and endoscopy for staging depth of invasion in early gastric cancer: a pilot study. Gastrointest Endosc. 1997;46:212–216. - PubMed
-
- Chung IK, Lee JH, Lee SH, Kim SJ, Cho JY, Cho WY, Hwangbo Y, Keum BR, Park JJ, Chun HJ, Kim HJ, Kim JJ, Ji SR, Seol SY. Therapeutic outcomes in 1000 cases of endoscopic submucosal dissection for early gastric neoplasms: Korean ESD Study Group multicenter study. Gastrointest Endosc. 2009;69:1228–1235. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
