

The Vascular Quality Initiative Cardiac Risk Index for prediction of myocardial infarction after vascular surgery
- PMID: 27449347
- PMCID: PMC5079798
- DOI: 10.1016/j.jvs.2016.04.045
The Vascular Quality Initiative Cardiac Risk Index for prediction of myocardial infarction after vascular surgery
Abstract
Objective: The objective of this study was to develop and to validate the Vascular Quality Initiative (VQI) Cardiac Risk Index (CRI) for prediction of postoperative myocardial infarction (POMI) after vascular surgery.
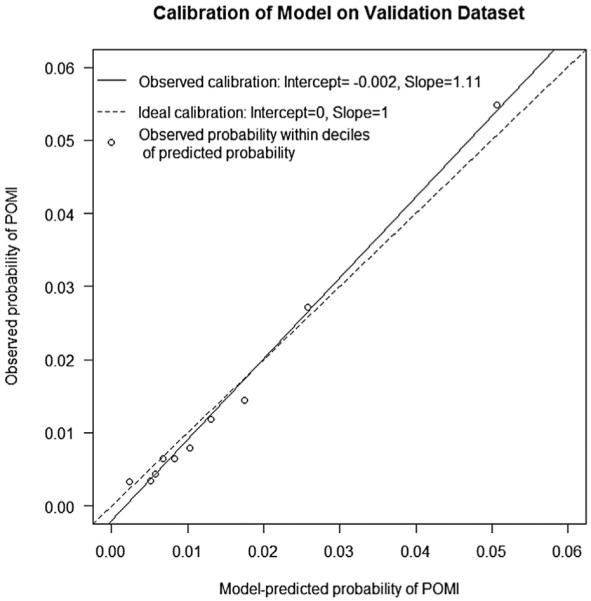
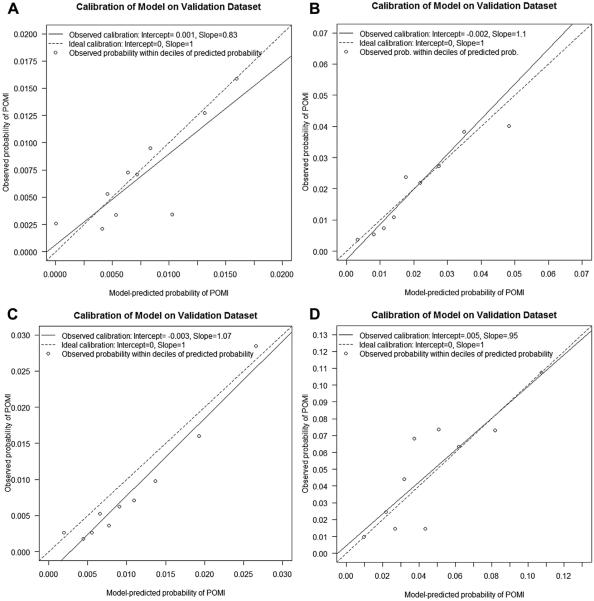
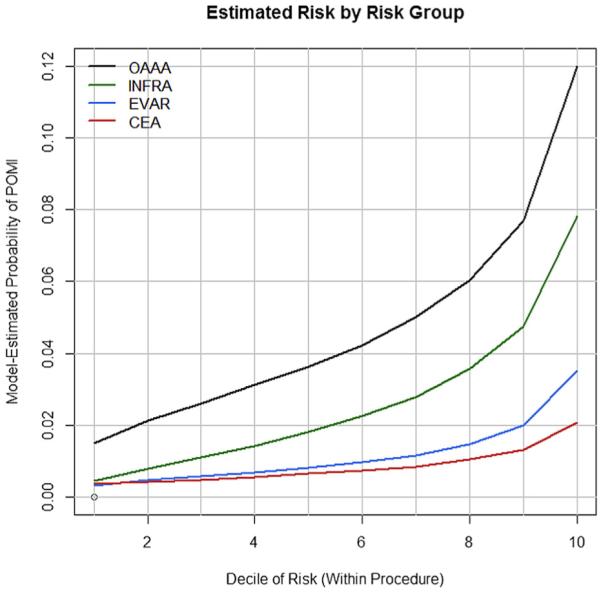
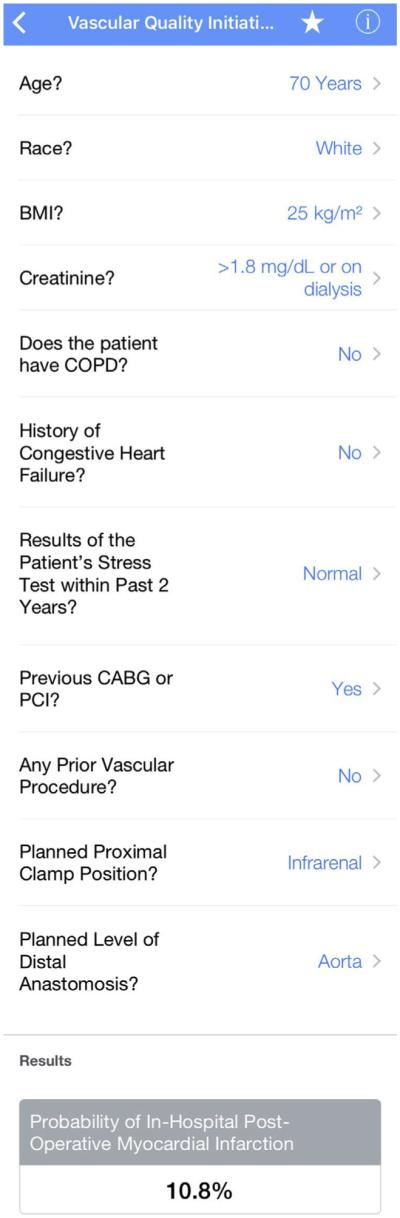
Methods: We developed risk models for in-hospital POMI after 88,791 nonemergent operations from the VQI registry, including carotid endarterectomy (CEA; n = 45,340), infrainguinal bypass (INFRA; n = 18,054), suprainguinal bypass (SUPRA; n = 2678), endovascular aneurysm repair (EVAR; n = 18,539), and open abdominal aortic aneurysm repair (OAAA repair; n = 4180). Multivariable logistic regression was used to create an all-procedure and four procedure-specific risk calculators based on the derivation cohort from 2012 to 2014 (N = 61,236). Generalizability of the all-procedure model was evaluated by applying it to each procedure subtype. The models were validated using a cohort (N = 27,555) from January 2015 to February 2016. Model discrimination was measured by area under the receiver operating characteristic curve (AUC), and performance was validated by bootstrapping 5000 iterations. The VQI CRI calculator was made available on the Internet and as a free smart phone app available through QxCalculate.
Results: Overall POMI incidence was 1.6%, with variation by procedure type as follows: CEA, 0.8%; EVAR, 1.0%; INFRA, 2.6%; SUPRA, 3.1%; and OAAA repair, 4.3% (P < .001). Predictors of POMI in the all-procedure model included age, operation type, coronary artery disease, congestive heart failure, diabetes, creatinine concentration >1.8 mg/dL, stress test status, and body mass index (AUC, 0.75; 95% confidence interval [CI], 0.73-0.76). The all-procedure model demonstrated only minimally reduced accuracy when it was applied to each procedure, with the following AUCs: CEA, 0.65 (95% CI, 0.59-0.70); INFRA, 0.69 (95% CI, 0.64-0.73); EVAR, 0.72 (95% CI, 0.65-0.80); SUPRA, 0.62 (95% CI, 0.52-0.72); and OAAA, 0.63 (95% CI, 0.56-0.70). Procedure-specific models had unique predictors and showed improved prediction compared with the all-procedure model, with the following AUCs: CEA, 0.69 (95% CI, 0.66-0.72); INFRA, 0.75 (95% CI, 0.73-0.78); EVAR, 0.76 (95% CI, 0.73-0.80); and OAAA, 0.72 (95% CI, 0.69-0.77). Bias-corrected AUC (95% CI) from internal validation for the models was as follows: all procedures, 0.75 (0.73-0.76); CEA, 0.68 (0.65-0.71); INFRA, 0.74 (0.72-0.76); EVAR, 0.73 (0.70-0.78); and OAAA repair, 0.68 (0.65-0.73).
Conclusions: The VQI CRI is a useful and valid clinical decision-making tool to predict POMI after vascular surgery. Procedure-specific models improve accuracy when they include unique risk factors.
Copyright © 2016 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Goldman L, Caldera DL, Nussbaum SR, Southwick FS, Krogstad D, Murray B, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med. 1977;297:845–50. - PubMed
-
- Detsky AS, Abrams HB, Forbath N, Scott JG, Hilliard JR. Cardiac assessment for patients undergoing noncardiac surgery. A multifactorial clinical risk index. Arch Intern Med. 1986;146:2131–4. - PubMed
-
- Kheterpal S, O’Reilly M, Englesbe MJ, Rosenberg AL, Shanks AM, Zhang L, et al. Preoperative and intraoperative predictors of cardiac adverse events after general, vascular, and urological surgery. Anesthesiology. 2009;110:58–66. - PubMed
-
- Cooperman M, Pflug B, Martin EW, Jr, Evans WE. Cardiovascular risk factors in patients with peripheral vascular disease. Surgery. 1978;84:505–9. - PubMed
-
- Yeager RA, Weigel RM, Murphy ES, McConnell DB, Sasaki TM, Vetto RM. Application of clinically valid cardiac risk factors to aortic aneurysm surgery. Arch Surg. 1986;121:278–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
