

Glioblastoma multiforme versus pleomorphic xanthoastrocytoma with anaplastic features in the pathological diagnosis: a case report
- PMID: 27449352
- PMCID: PMC4957929
- DOI: 10.1186/s13000-016-0514-2
Glioblastoma multiforme versus pleomorphic xanthoastrocytoma with anaplastic features in the pathological diagnosis: a case report
Abstract
Background: Pleomorphic xanthoastrocytoma (PXA) with anaplastic features should be strictly distinguished from glioblastoma multiforme (GBM).
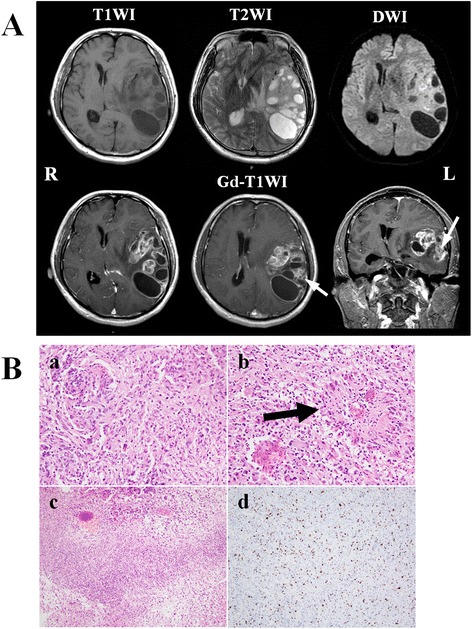
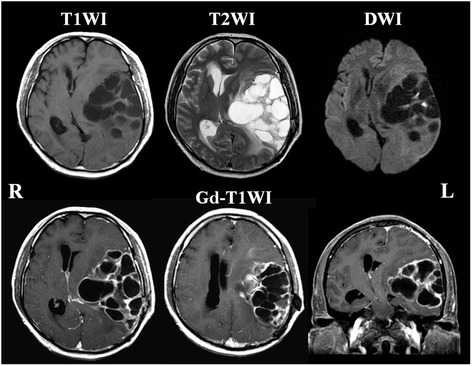
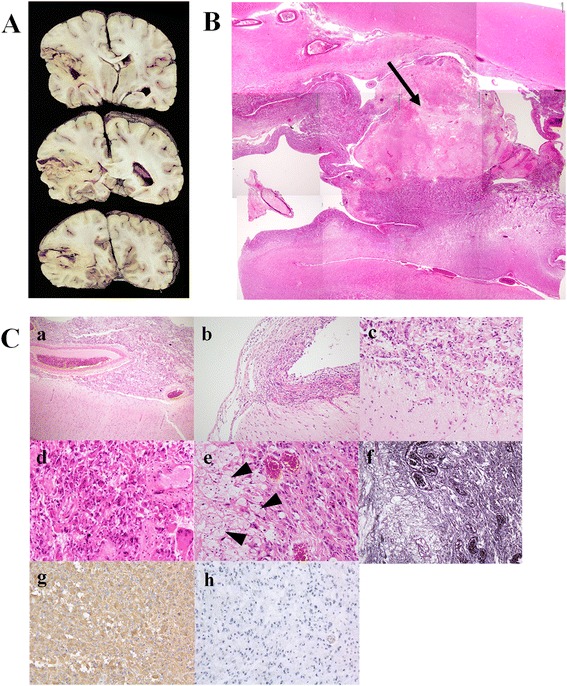
Case presentation: A case of PXA that was initially diagnosed as GBM is presented. A 42-year-old man visited our clinic because of right hemiparesis and total aphasia. Head magnetic resonance imaging demonstrated enhanced multiple cystic lesions in the left temporal lobe suggesting an intra-parenchymal brain tumor. The lesion was partially removed and GBM with a Ki-67 index of 20 % was diagnosed by pathological examination of the resected specimen. Despite receiving radiation and chemotherapy, the patient died 6 months after the first admission. At autopsy, the boundary between the tumor and normal brain tissue was clear. Large parts of the tumor demonstrated typical features of PXA, including pleomorphism, clear xanthomatous cells with foamy cytoplasm, positive silver staining, and a Ki-67 index of less than 1 %.
Discussion and conclusions: GBM should be diagnosed only when the majority of the tumor cells are undifferentiated. Although the operative specimen appeared typical GBM histologically, the diagnosis of GBM was subsequently excluded by the autopsy finding that much of the tumor had the characteristic features of a benign PXA. Therefore, the final diagnosis in this case was PXA with anaplastic features. PXA with anaplastic features should be carefully distinguished from GBM to facilitate appropriate decisions concerning treatment.
Keywords: Anaplastic features; Glioblastoma; Ki-67 index; Pleomorphic xanthoastrocytoma.
Figures
Similar articles
-
Malignant transformation of pleomorphic xanthoastrocytoma and differential diagnosis: case report.BMC Neurol. 2020 Jan 15;20(1):21. doi: 10.1186/s12883-020-1601-2. BMC Neurol. 2020. PMID: 31941461 Free PMC article.
-
A case of anaplastic pleomorphic xanthoastrocytoma presenting with tumor bleeding and cerebrospinal fluid dissemination.Brain Tumor Pathol. 2006 Apr;23(1):55-63. doi: 10.1007/s10014-006-0197-6. Brain Tumor Pathol. 2006. PMID: 18095120
-
Pleomorphic xanthoastrocytoma in elderly patients may portend a poor prognosis.J Clin Neurosci. 2008 Apr;15(4):476-8. doi: 10.1016/j.jocn.2006.09.012. Epub 2008 Feb 6. J Clin Neurosci. 2008. PMID: 18255294
-
Malignant progression in pleomorphic xanthoastrocytoma: personal experience and review of the literature.J Neurol Sci. 2007 Jan 31;252(2):144-53. doi: 10.1016/j.jns.2006.11.008. Epub 2006 Dec 26. J Neurol Sci. 2007. PMID: 17189643 Review.
-
Pleomorphic xanthoastrocytoma, anaplastic pleomorphic xanthoastrocytoma, and epithelioid glioblastoma: Case series with clinical characteristics, molecular features and progression relationship.Clin Neurol Neurosurg. 2022 Oct;221:107379. doi: 10.1016/j.clineuro.2022.107379. Epub 2022 Jul 21. Clin Neurol Neurosurg. 2022. PMID: 35932588 Review.
Cited by
-
Clinical features and surgical outcomes of high grade pleomorphic xanthoastrocytomas: a single-center experience with a systematic review.Front Oncol. 2023 Jun 28;13:1193611. doi: 10.3389/fonc.2023.1193611. eCollection 2023. Front Oncol. 2023. PMID: 37448517 Free PMC article.
-
Malignant transformation of pleomorphic xanthoastrocytoma in pregnant patient: Clinical case and ethical dilemma.Surg Neurol Int. 2021 Sep 20;12:469. doi: 10.25259/SNI_120_2021. eCollection 2021. Surg Neurol Int. 2021. PMID: 34621584 Free PMC article.
-
Intraoperative Frozen Cytology of Central Nervous System Neoplasms: An Ancillary Tool for Frozen Diagnosis.J Pathol Transl Med. 2019 Mar;53(2):104-111. doi: 10.4132/jptm.2018.11.10. Epub 2019 Jan 14. J Pathol Transl Med. 2019. PMID: 30636391 Free PMC article.
-
Demography, Pattern of Care, and Survival in Patients with Xanthoastrocytoma: A Systematic Review and Individual Patient Data Analysis of 325 Cases.J Neurosci Rural Pract. 2019 Jul;10(3):430-437. doi: 10.1055/s-0039-1697873. Epub 2019 Oct 7. J Neurosci Rural Pract. 2019. PMID: 31595115 Free PMC article.
-
Malignant transformation of pleomorphic xanthoastrocytoma and differential diagnosis: case report.BMC Neurol. 2020 Jan 15;20(1):21. doi: 10.1186/s12883-020-1601-2. BMC Neurol. 2020. PMID: 31941461 Free PMC article.
References
-
- Tihan T. Proliferation markers in the evaluation of gliomas. In: Winn RH, editor. Youman’s neurological surgery. 6. Philadelphia: Elsevier Saunders; 2011. pp. 1108–1111.
-
- Weldon-Linne CM, Victor TA, Groothuis DR, Vick NA. Pleomorphic xanthoastrocytoma. Ultrastructural and immunohistochemical study of a case with a rapidly fatal outcome following surgery. Cancer. 1983;52:2055–2063. doi: 10.1002/1097-0142(19831201)52:11<2055::AID-CNCR2820521115>3.0.CO;2-W. - DOI - PubMed
-
- Giannini C, Scheithauer BW, Burger PC, Brat DJ, Wollan PC, Lach B, et al. Pleomorphic xanthoastrocytoma: what do we really know about it? Cancer. 1999;85:2033–45. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
