

Recommendations for the Prophylactic Management of Skin Reactions Induced by Epidermal Growth Factor Receptor Inhibitors in Patients With Solid Tumors
- PMID: 27449521
- PMCID: PMC5153350
- DOI: 10.1634/theoncologist.2016-0051
Recommendations for the Prophylactic Management of Skin Reactions Induced by Epidermal Growth Factor Receptor Inhibitors in Patients With Solid Tumors
Abstract
: Inhibition of the epidermal growth factor receptor (EGFR) is an established treatment that extends patient survival across a variety of tumor types. EGFR inhibitors fall into two main categories: anti-EGFR monoclonal antibodies, such as cetuximab and panitumumab, and first-generation tyrosine kinase inhibitors, such as afatinib, gefitinib, and erlotinib. Skin reactions are the most common EGFR inhibitor-attributable adverse event, resulting in papulopustular (acneiform) eruptions that can be painful and debilitating, and which may potentially have a negative impact on patients' quality of life and social functioning, as well as a negative impact on treatment duration. Shortened treatment duration can, in turn, compromise antineoplastic efficacy. Similarly, appropriate management of skin reactions is dependent on their accurate grading; however, conventional means for grading skin reactions are inadequate, particularly within the context of clinical trials. Treating a skin reaction only once it occurs (reactive treatment strategies) may not be the most effective management approach; instead, prophylactic approaches may be preferable. Indeed, we support the viewpoint that prophylactic management of skin reactions should be recommended for all patients treated with EGFR inhibitors. Appropriate prophylactic management could effectively reduce the severity of skin reactions in patients treated with EGFR inhibitors and therefore has the potential to directly benefit patients and improve drug adherence. Accordingly, here we review published and still-emerging data, and provide practical and evidence-based recommendations and algorithms regarding the optimal prophylactic management of EGFR inhibitor-attributable skin reactions.
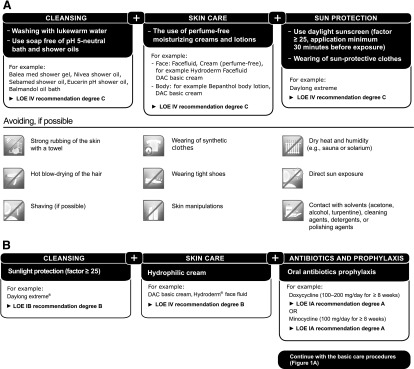
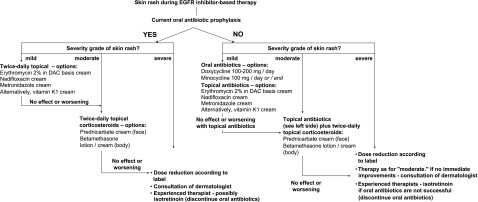
Implications for practice: Epidermal growth factor receptor (EGFR) inhibitors extend patient survival across a variety of tumor types. The most common EGFR inhibitor-attributable adverse events are skin reactions. Prophylactic-rather than reactive-management of skin reactions for all patients receiving EGFR inhibitors should be recommended because appropriate prophylaxis could effectively reduce the severity of skin reactions; thus, the derivation of highly effective prophylactic strategies has the potential to directly benefit patients. Accordingly, a review of the available data leads to practical and evidence-based recommendations and algorithms regarding the optimal prophylactic management of EGFR inhibitor-attributable skin reactions.
Keywords: Algorithms; EGFR inhibitors; Prophylactic care; Skin reactions.
©AlphaMed Press.
Conflict of interest statement
of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Van Cutsem E, Köhne CH, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360:1408–1417. - PubMed
-
- Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med. 2006;354:567–578. - PubMed
-
- Pirker R, Pereira JR, Szczesna A, et al. Cetuximab plus chemotherapy in patients with advanced non-small-cell lung cancer (FLEX): An open-label randomised phase III trial. Lancet. 2009;373:1525–1531. - PubMed
-
- Moore MJ, Goldstein D, Hamm J, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: A phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 2007;25:1960–1966. - PubMed
-
- Vermorken JB, Mesia R, Rivera F, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med. 2008;359:1116–1127. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
