

Comparison of Urine Output among Patients Treated with More Intensive Versus Less Intensive RRT: Results from the Acute Renal Failure Trial Network Study
- PMID: 27449661
- PMCID: PMC4974887
- DOI: 10.2215/CJN.10991015
Comparison of Urine Output among Patients Treated with More Intensive Versus Less Intensive RRT: Results from the Acute Renal Failure Trial Network Study
Abstract
Background and objectives: Intensive RRT may have adverse effects that account for the absence of benefit observed in randomized trials of more intensive versus less intensive RRT. We wished to determine the association of more intensive RRT with changes in urine output as a marker of worsening residual renal function in critically ill patients with severe AKI.
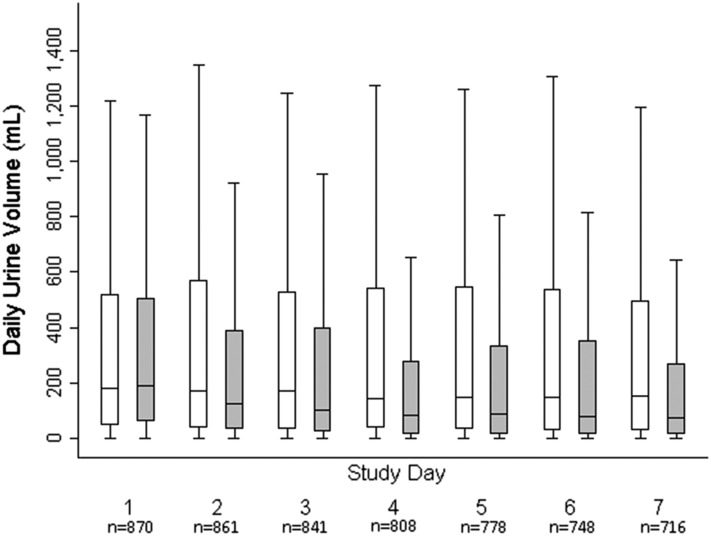
Design, setting, participants, & measurements: The Acute Renal Failure Trial Network Study (n=1124) was a multicenter trial that randomized critically ill patients requiring initiation of RRT to more intensive (hemodialysis or sustained low-efficiency dialysis six times per week or continuous venovenous hemodiafiltration at 35 ml/kg per hour) versus less intensive (hemodialysis or sustained low-efficiency dialysis three times per week or continuous venovenous hemodiafiltration at 20 ml/kg per hour) RRT. Mixed linear regression models were fit to estimate the association of RRT intensity with change in daily urine output in survivors through day 7 (n=871); Cox regression models were fit to determine the association of RRT intensity with time to ≥50% decline in urine output in all patients through day 28.
Results: Mean age of participants was 60±15 years old, 72% were men, and 30% were diabetic. In unadjusted models, among patients who survived ≥7 days, mean urine output was, on average, 31.7 ml/d higher (95% confidence interval, 8.2 to 55.2 ml/d) for the less intensive group compared with the more intensive group (P=0.01). More intensive RRT was associated with 29% greater unadjusted risk of decline in urine output of ≥50% (hazard ratio, 1.29; 95% confidence interval, 1.10 to 1.51).
Conclusions: More intensive versus less intensive RRT is associated with a greater reduction in urine output during the first 7 days of therapy and a greater risk of developing a decline in urine output of ≥50% in critically ill patients with severe AKI.
Keywords: Acute kidney injury; Humans; Randomized trials as topic; critical illness; hemodialysis; renal dialysis; renal replacement therapy.
Copyright © 2016 by the American Society of Nephrology.
Figures

Comment in
-
Does Changing the Volume Matter? The Relationship of Urine Volume and Dialysis Intensity.Clin J Am Soc Nephrol. 2016 Aug 8;11(8):1321-1323. doi: 10.2215/CJN.06420616. Epub 2016 Jul 22. Clin J Am Soc Nephrol. 2016. PMID: 27449662 Free PMC article. No abstract available.
-
More May be Less; Yet Another Way which More Intense Renal Replacement Therapy May Not be Better.Semin Dial. 2016 Nov;29(6):515-517. doi: 10.1111/sdi.12556. Epub 2016 Oct 10. Semin Dial. 2016. PMID: 27726171 No abstract available.
References
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C; Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators : Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA 294: 813–818, 2005 - PubMed
-
- Turney JH, Marshall DH, Brownjohn AM, Ellis CM, Parsons FM: The evolution of acute renal failure, 1956-1988. Q J Med 74: 83–104, 1990 - PubMed
-
- Ronco C, Bellomo R, Homel P, Brendolan A, Dan M, Piccinni P, La Greca G: Effects of different doses in continuous veno-venous haemofiltration on outcomes of acute renal failure: A prospective randomised trial. Lancet 356: 26–30, 2000 - PubMed
-
- Saudan P, Niederberger M, De Seigneux S, Romand J, Pugin J, Perneger T, Martin PY: Adding a dialysis dose to continuous hemofiltration increases survival in patients with acute renal failure. Kidney Int 70: 1312–1317, 2006 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
