

Idiopathic hypercalciuria and formation of calcium renal stones
- PMID: 27452364
- PMCID: PMC5837277
- DOI: 10.1038/nrneph.2016.101
Idiopathic hypercalciuria and formation of calcium renal stones
Abstract
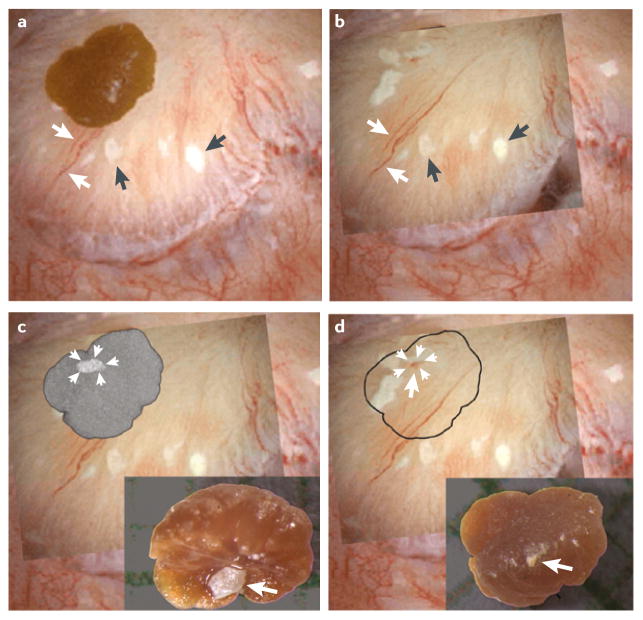
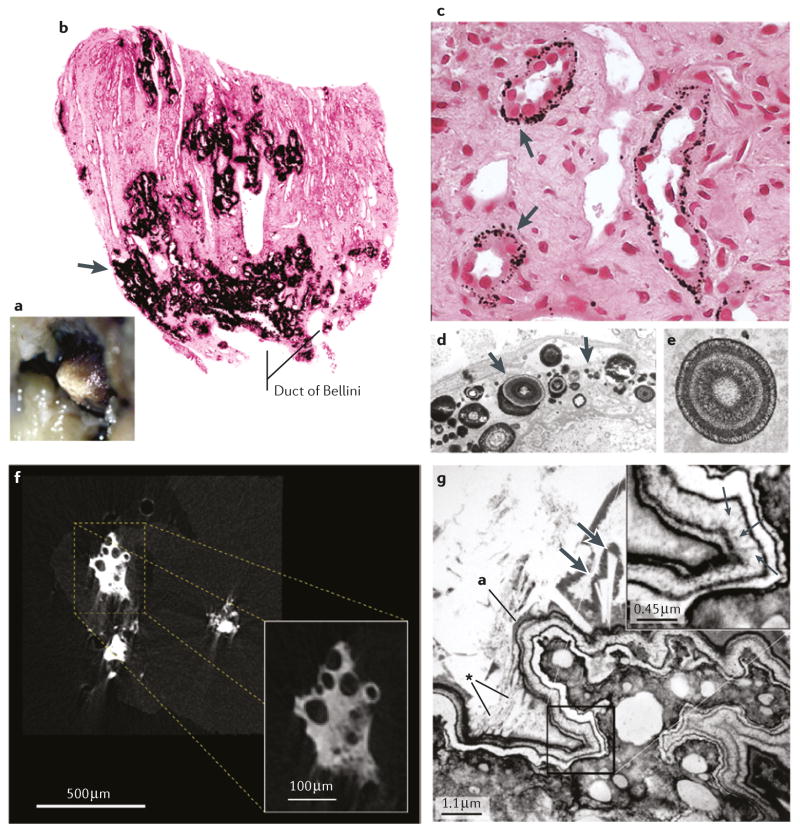
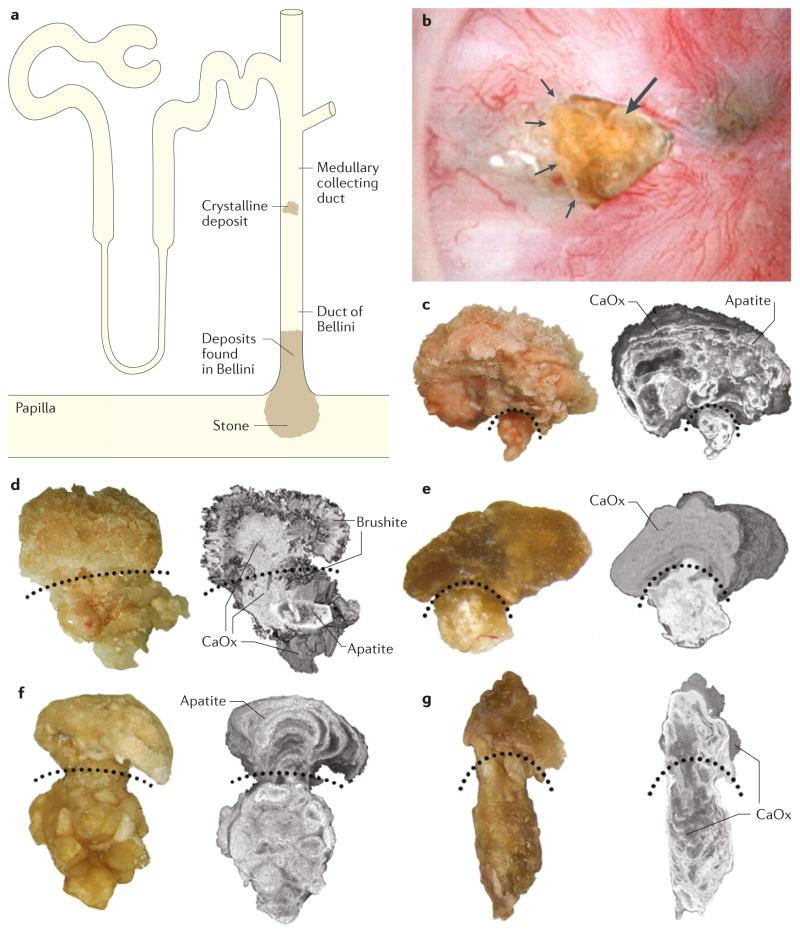
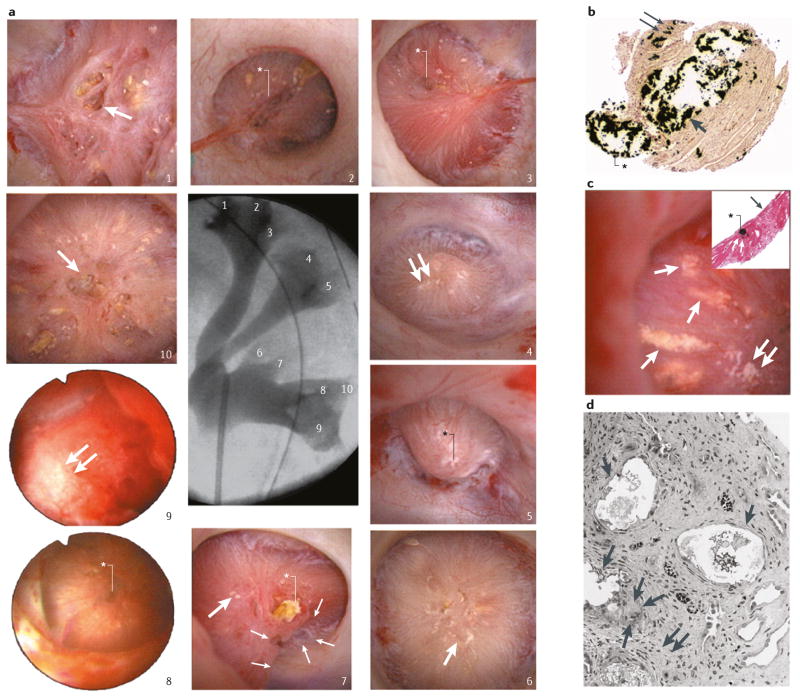
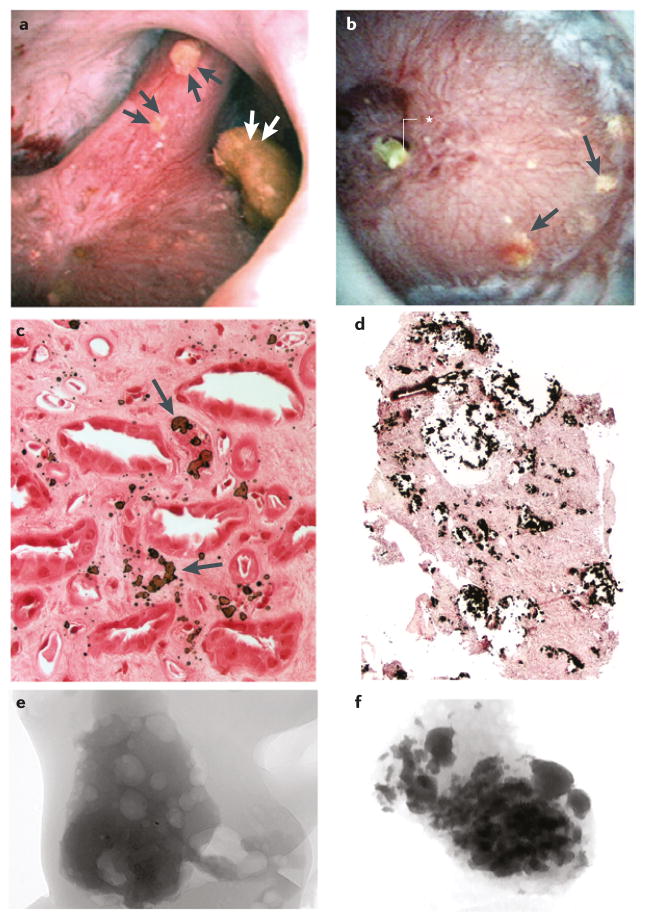
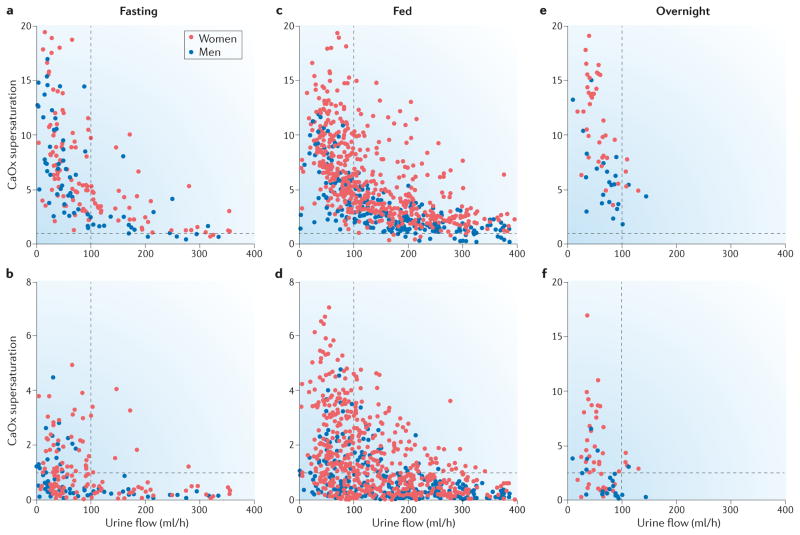
The most common presentation of nephrolithiasis is idiopathic calcium stones in patients without systemic disease. Most stones are primarily composed of calcium oxalate and form on a base of interstitial apatite deposits, known as Randall's plaque. By contrast some stones are composed largely of calcium phosphate, as either hydroxyapatite or brushite (calcium monohydrogen phosphate), and are usually accompanied by deposits of calcium phosphate in the Bellini ducts. These deposits result in local tissue damage and might serve as a site of mineral overgrowth. Stone formation is driven by supersaturation of urine with calcium oxalate and brushite. The level of supersaturation is related to fluid intake as well as to the levels of urinary citrate and calcium. Risk of stone formation is increased when urine citrate excretion is <400 mg per day, and treatment with potassium citrate has been used to prevent stones. Urine calcium levels >200 mg per day also increase stone risk and often result in negative calcium balance. Reduced renal calcium reabsorption has a role in idiopathic hypercalciuria. Low sodium diets and thiazide-type diuretics lower urine calcium levels and potentially reduce the risk of stone recurrence and bone disease.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Parks JH, Worcester EM, Coe FL, Evan AP, Lingeman JE. Clinical implications of abundant calcium phosphate in routinely analyzed kidney stones. Kidney Int. 2004;66:777–785. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
