

Estimating Ten-Year Trends in Septic Shock Incidence and Mortality in United States Academic Medical Centers Using Clinical Data
- PMID: 27452768
- PMCID: PMC5310115
- DOI: 10.1016/j.chest.2016.07.010
Estimating Ten-Year Trends in Septic Shock Incidence and Mortality in United States Academic Medical Centers Using Clinical Data
Abstract
Background: Reports that septic shock incidence is rising and mortality rates declining may be confounded by improving recognition of sepsis and changing coding practices. We compared trends in septic shock incidence and mortality in academic hospitals using clinical vs claims data.
Methods: We identified all patients with concurrent blood cultures, antibiotics, and vasopressors for ≥ two consecutive days, and all patients with International Classification of Diseases, 9th edition (ICD-9) codes for septic shock, at 27 academic hospitals from 2005 to 2014. We compared annual incidence and mortality trends. We reviewed 967 records from three hospitals to estimate the accuracy of each method.
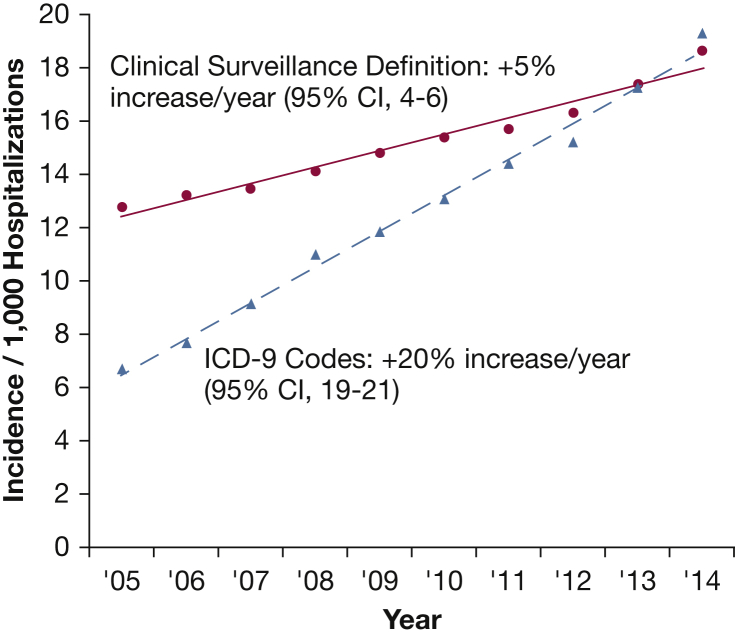
Results: Of 6.5 million adult hospitalizations, 99,312 (1.5%) were flagged by clinical criteria, 82,350 (1.3%) by ICD-9 codes, and 44,651 (0.7%) by both. Sensitivity for clinical criteria was higher than claims (74.8% vs 48.3%; P < .01), whereas positive predictive value was comparable (83% vs 89%; P = .23). Septic shock incidence, based on clinical criteria, rose from 12.8 to 18.6 cases per 1,000 hospitalizations (average, 4.9% increase/y; 95% CI, 4.0%-5.9%), while mortality declined from 54.9% to 50.7% (average, 0.6% decline/y; 95% CI, 0.4%-0.8%). In contrast, septic shock incidence, based on ICD-9 codes, increased from 6.7 to 19.3 per 1,000 hospitalizations (19.8% increase/y; 95% CI, 16.6%-20.9%), while mortality decreased from 48.3% to 39.3% (1.2% decline/y; 95% CI, 0.9%-1.6%).
Conclusions: A clinical surveillance definition based on concurrent vasopressors, blood cultures, and antibiotics accurately identifies septic shock hospitalizations and suggests that the incidence of patients receiving treatment for septic shock has risen and mortality rates have fallen, but less dramatically than estimated on the basis of ICD-9 codes.
Keywords: epidemiology; incidence; mortality; sepsis; septic shock; trends.
Copyright © 2016 American College of Chest Physicians. All rights reserved.
Figures


Comment in
-
Septic Shock Surveillance: Critically Important but Not Straightforward.Chest. 2017 Feb;151(2):247-248. doi: 10.1016/j.chest.2016.08.1433. Chest. 2017. PMID: 28183481 No abstract available.
References
-
- Bone R.C., Balk R.A., Cerra F.B., ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101(6):1644–1655. As cited in Tillotson GS. Introduction: sepsis. Chest. 2009;136(5 suppl):e28. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
