

Continuity of Care and Health Care Utilization in Older Adults With Dementia in Fee-for-Service Medicare
- PMID: 27454945
- PMCID: PMC5061498
- DOI: 10.1001/jamainternmed.2016.3553
Continuity of Care and Health Care Utilization in Older Adults With Dementia in Fee-for-Service Medicare
Abstract
Importance: Poor continuity of care may contribute to high health care spending and adverse patient outcomes in dementia.
Objective: To examine the association between medical clinician continuity and health care utilization, testing, and spending in older adults with dementia.
Design, setting, and participants: This was a study of an observational retrospective cohort from the 2012 national sample in fee-for-service Medicare, conducted from July to December 2015, using inverse probability weighted analysis. A total of 1 416 369 continuously enrolled, community-dwelling, fee-for-service Medicare beneficiaries 65 years or older with a claims-based dementia diagnosis and at least 4 ambulatory visits in 2012 were included.
Exposures: Continuity of care score measured on patient visits across physicians over 12 months. A higher continuity score is assigned to visit patterns in which a larger share of the patient's total visits are with fewer clinicians. Score range from 0 to 1 was examined in low-, medium-, and high-continuity tertiles.
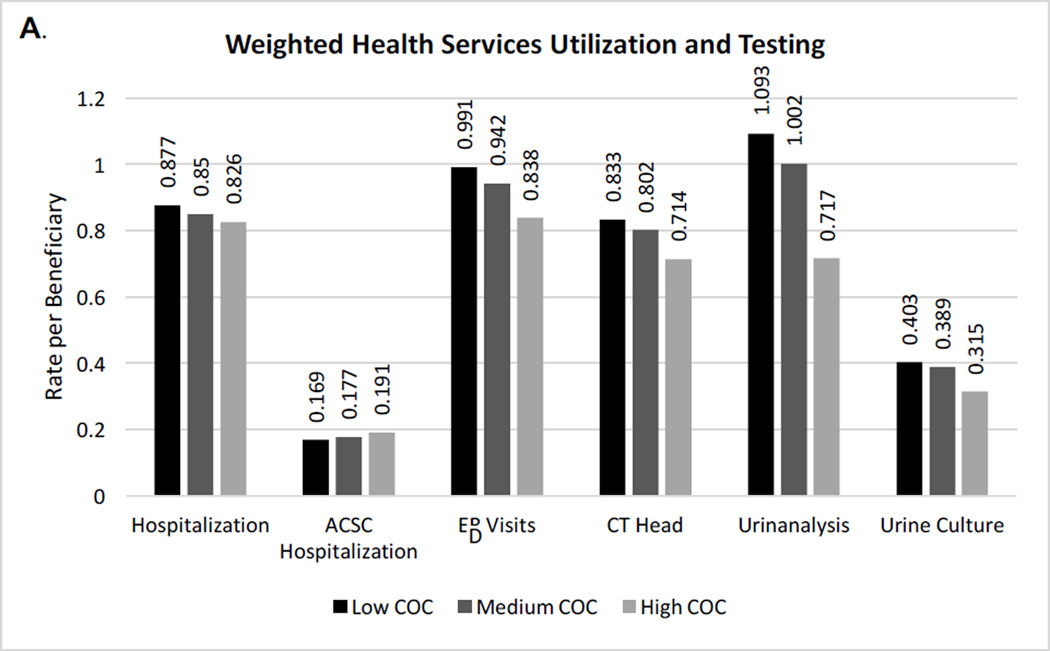
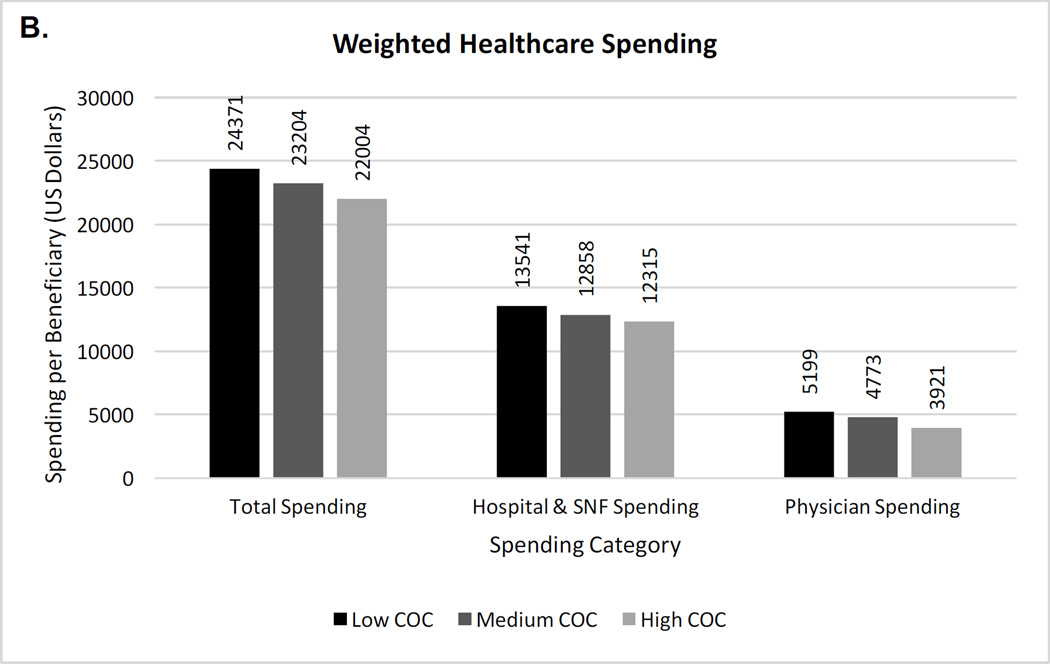
Main outcomes and measures: Outcomes include all-cause hospitalization, ambulatory care sensitive condition hospitalization, emergency department visit, imaging, and laboratory testing (computed tomographic [CT] scan of the head, chest radiography, urinalysis, and urine culture), and health care spending (overall, hospital and skilled nursing facility, and physician).
Results: Beneficiaries with dementia who had lower levels of continuity of care were younger, had a higher income, and had more comorbid medical conditions. Almost 50% of patients had at least 1 hospitalization and emergency department visit during the year. Utilization was lower with increasing level of continuity. Specifically comparing the highest- vs lowest-continuity groups, annual rates per beneficiary of hospitalization (0.83 vs 0.88), emergency department visits (0.84 vs 0.99), CT scan of the head (0.71 vs 0.83), urinalysis (0.72 vs 1.09), and health care spending (total spending, $22 004 vs $24 371) were higher with lower continuity even after accounting for sociodemographic factors and comorbidity burden (P < .001 for all comparisons). The rate of ambulatory care sensitive condition hospitalization was similar across continuity groups.
Conclusions and relevance: Among older fee-for-service Medicare beneficiaries with a dementia diagnosis, lower continuity of care is associated with higher rates of hospitalization, emergency department visits, testing, and health care spending. Further research into these relationships, including potentially relevant clinical, clinician, and systems factors, can inform whether improving continuity of care in this population may benefit patients and the wider health system.
Conflict of interest statement
Disclosures: None.
Figures
Comment in
-
Medical Care When Memory Fails.JAMA Intern Med. 2016 Sep 1;176(9):1378-9. doi: 10.1001/jamainternmed.2016.3566. JAMA Intern Med. 2016. PMID: 27454073 No abstract available.
References
-
- Bynum JP. The long reach of Alzheimer’s disease: Patients, practice, and policy. Health Aff (Millwood) 2014;33(4):534–540. - PubMed
-
- Bynum JP, Rabins PV, Weller W, Niefeld M, Anderson GF, Wu AW. The relationship between a dementia diagnosis, chronic illness, Medicare expenditures, and hospital use. J Am Geriatr Soc. 2004;52(2):187–194. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
