

Does Anticoagulant Medication Alter Fracture-Healing? A Morphological and Biomechanical Evaluation of the Possible Effects of Rivaroxaban and Enoxaparin Using a Rat Closed Fracture Model
- PMID: 27455072
- PMCID: PMC4959754
- DOI: 10.1371/journal.pone.0159669
Does Anticoagulant Medication Alter Fracture-Healing? A Morphological and Biomechanical Evaluation of the Possible Effects of Rivaroxaban and Enoxaparin Using a Rat Closed Fracture Model
Abstract
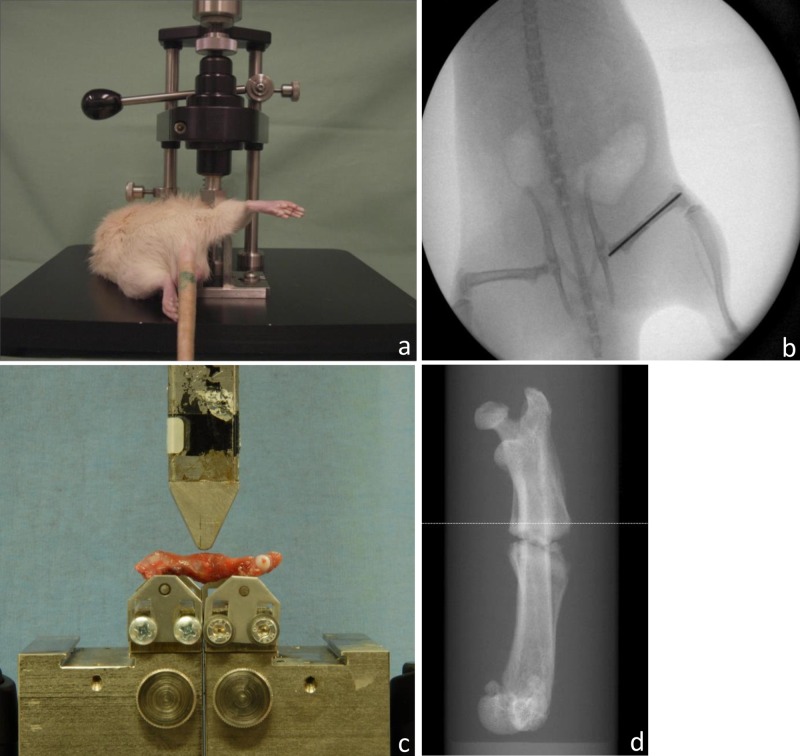
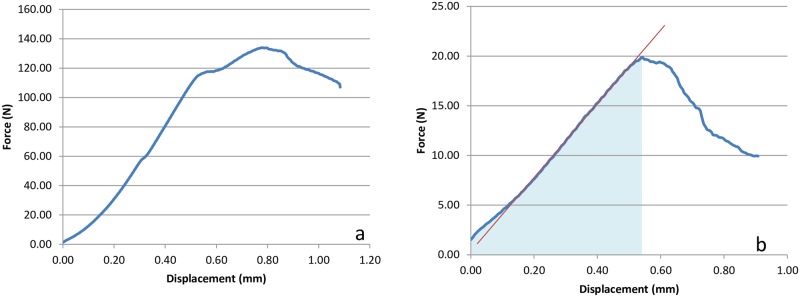
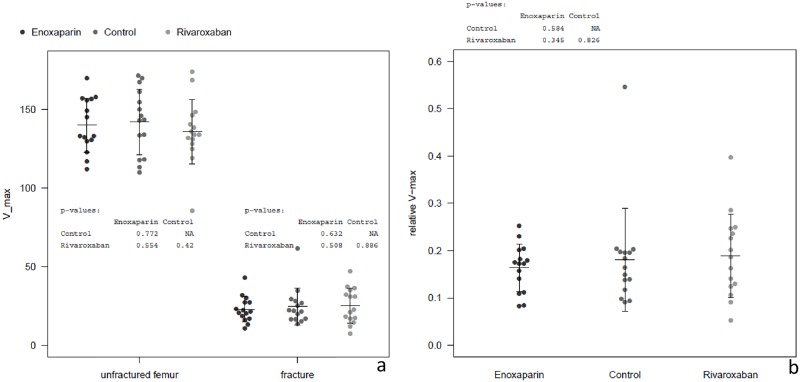
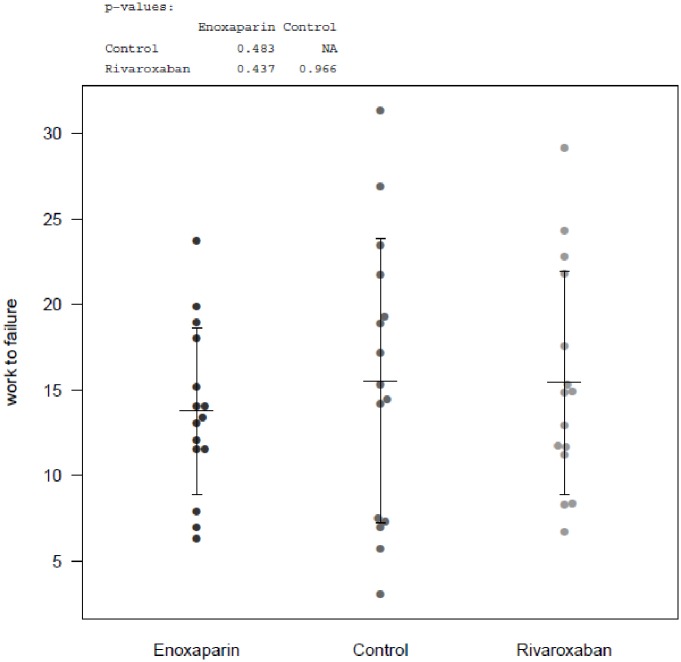
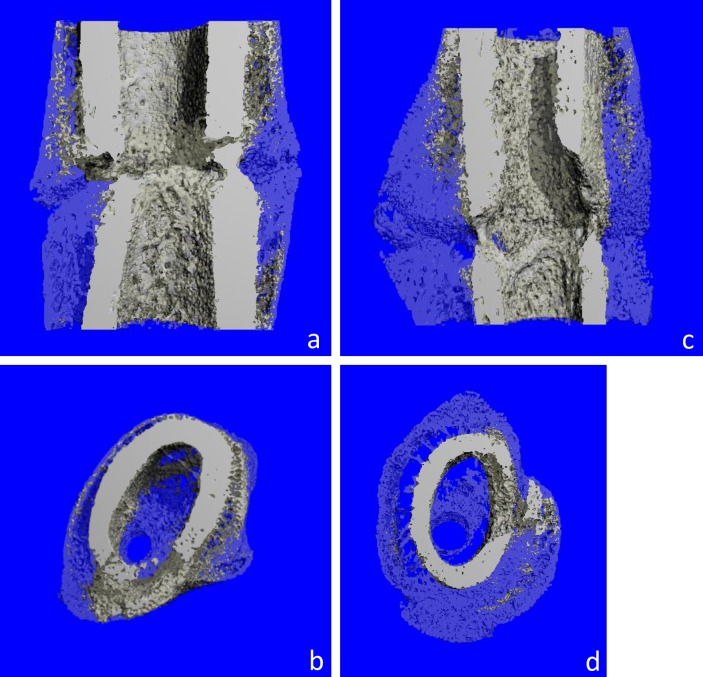
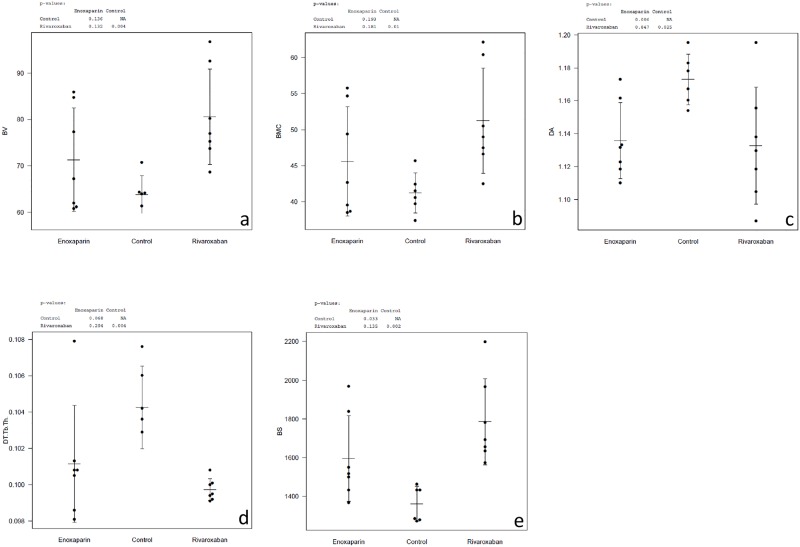
Low molecular weight heparin (LMWH) is routinely used to prevent thromboembolism in orthopaedic surgery, especially in the treatment of fractures or after joint-replacement. Impairment of fracture-healing due to increased bone-desorption, delayed remodelling and lower calcification caused by direct osteoclast stimulation is a well-known side effect of unfractioned heparin. However, the effect of LMWH is unclear and controversial. Recent studies strongly suggest impairment of bone-healing in-vitro and in animal models, characterized by a significant decrease in volume and quality of new-formed callus. Since October 2008, Rivaroxaban (Xarelto) is available for prophylactic use in elective knee- and hip-arthroplasty. Recently, some evidence has been found indicating an in vitro dose independent reduction of osteoblast function after Rivaroxaban treatment. In this study, the possible influence of Rivaroxaban and Enoxaparin on bone-healing in vivo was studied using a standardized, closed rodent fracture-model. 70 male Wistar-rats were randomized to Rivaroxaban, Enoxaparin or control groups. After pinning the right femur, a closed, transverse fracture was produced. 21 days later, the animals were sacrificed and both femora harvested. Analysis was done by biomechanical testing (three-point bending) and micro CT. Both investigated substances showed histomorphometric alterations of the newly formed callus assessed by micro CT analysis. In detail the bone (callus) volume was enhanced (sign. for Rivaroxaban) and the density reduced. The bone mineral content was enhanced accordingly (sign. for Rivaroxaban). Trabecular thickness was reduced (sign. for Rivaroxaban). Furthermore, both drugs showed significant enlarged bone (callus) surface and degree of anisotropy. In contrast, the biomechanical properties of the treated bones were equal to controls. To summarize, the morphological alterations of the fracture-callus did not result in functionally relevant deficits.
Conflict of interest statement
Figures
References
-
- Colwell CW Jr. Rationale for thromboprophylaxis in lower joint arthroplasty. Am J Orthop (Belle Mead NJ). 2007;36(9 Suppl):11–3. Epub 2007/12/06. . - PubMed
-
- Turpie AG. Efficacy of a postoperative regimen of enoxaparin in deep vein thrombosis prophylaxis. Am J Surg. 1991;161(4):532–6. Epub 1991/04/01. 0002-9610(91)91126-4 [pii]. . - PubMed
-
- Eriksson BI, Kakkar AK, Turpie AG, Gent M, Bandel TJ, Homering M, et al. Oral rivaroxaban for the prevention of symptomatic venous thromboembolism after elective hip and knee replacement. J Bone Joint Surg Br. 2009;91(5):636–44. Epub 2009/05/02. 91-B/5/636 [pii] 10.1302/0301-620X.91B5.21691 . - DOI - PubMed
-
- Stinchfield FE, Sankaran B, Samilson R. The effect of anticoagulant therapy on bone repair. J Bone Joint Surg Am. 1956;38-A(2):270–82. Epub 1956/04/01. . - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
