

Primary Stroke Center Hospitalization for Elderly Patients With Stroke: Implications for Case Fatality and Travel Times
- PMID: 27455403
- PMCID: PMC5434865
- DOI: 10.1001/jamainternmed.2016.3919
Primary Stroke Center Hospitalization for Elderly Patients With Stroke: Implications for Case Fatality and Travel Times
Abstract
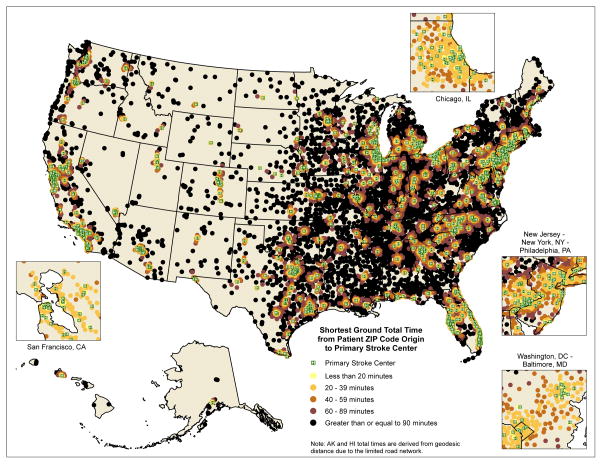
Importance: Physicians often must decide whether to treat patients with acute stroke locally or refer them to a more distant Primary Stroke Center (PSC). There is little evidence on how much the increased risk of prolonged travel time offsets benefits of a specialized PSC care.
Objectives: To examine the association of case fatality with receiving care in PSCs vs other hospitals for patients with stroke and to identify whether prolonged travel time offsets the effect of PSCs.
Design, setting, and participants: Retrospective cohort study of Medicare beneficiaries with stroke admitted to a hospital between January 1, 2010, and December 31, 2013. Drive times were calculated based on zip code centroids and street-level road network data. We used an instrumental variable analysis based on the differential travel time to PSCs to control for unmeasured confounding. The setting was a 100% sample of Medicare fee-for-service claims.
Exposures: Admission to a PSC.
Main outcomes and measures: Seven-day and 30-day postadmission case-fatality rates.
Results: Among 865 184 elderly patients with stroke (mean age, 78.9 years; 55.5% female), 53.9% were treated in PSCs. We found that admission to PSCs was associated with 1.8% (95% CI, -2.1% to -1.4%) lower 7-day and 1.8% (95% CI, -2.3% to -1.4%) lower 30-day case fatality. Fifty-six patients with stroke needed to be treated in PSCs to save one life at 30 days. Receiving treatment in PSCs was associated with a 30-day survival benefit for patients traveling less than 90 minutes, but traveling at least 90 minutes offset any benefit of PSC care.
Conclusions and relevance: Hospitalization of patients with stroke in PSCs was associated with decreased 7-day and 30-day case fatality compared with noncertified hospitals. Traveling at least 90 minutes to receive care offset the 30-day survival benefit of PSC admission.
Figures
Comment in
-
Admitting the Patient With Acute Stroke to the Right House-Lessons From the Sorting Hat of Hogwarts.JAMA Intern Med. 2016 Sep 1;176(9):1368-70. doi: 10.1001/jamainternmed.2016.3930. JAMA Intern Med. 2016. PMID: 27454422 No abstract available.
References
-
- Centers for Disease Control and Prevention (CDC) Prevalence of Stroke — United States, 2006–2010. MMWR Morb Mortal Wkly Rep. 2012;61(20):379–382. - PubMed
-
- Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010;121(7):e46–e215. - PubMed
-
- Schellinger PD, Köhrmann M. 4.5-hour time window for intravenous thrombolysis with recombinant tissue-type plasminogen activator is established firmly. Stroke. 2014;45(3):912–913. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
