

Pilot study to test the feasibility of a trial design and complex intervention on PRIoritising MUltimedication in Multimorbidity in general practices (PRIMUMpilot)
- PMID: 27456328
- PMCID: PMC4964238
- DOI: 10.1136/bmjopen-2016-011613
Pilot study to test the feasibility of a trial design and complex intervention on PRIoritising MUltimedication in Multimorbidity in general practices (PRIMUMpilot)
Abstract
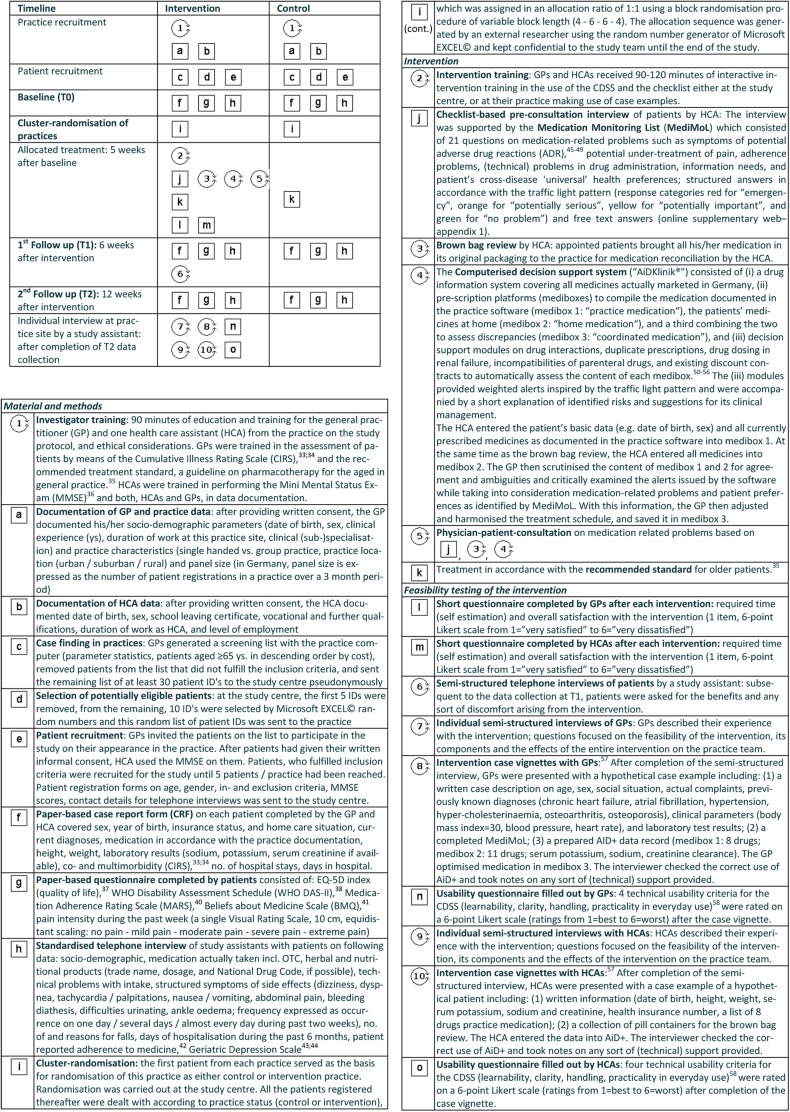
Objective: To improve medication appropriateness and adherence in elderly patients with multimorbidity, we developed a complex intervention involving general practitioners (GPs) and their healthcare assistants (HCA). In accordance with the Medical Research Council guidance on developing and evaluating complex interventions, we prepared for the main study by testing the feasibility of the intervention and study design in a cluster randomised pilot study.
Setting: 20 general practices in Hesse, Germany.
Participants: 100 cognitively intact patients ≥65 years with ≥3 chronic conditions, ≥5 chronic prescriptions and capable of participating in telephone interviews; 94 patients completed the study.
Intervention: The HCA conducted a checklist-based interview with patients on medication-related problems and reconciled their medications. Assisted by a computerised decision-support system (CDSS), the GPs discussed medication intake with patients and adjusted their medication regimens. The control group continued with usual care.
Outcome measures: Feasibility of the intervention and required time were assessed for GPs, HCAs and patients using mixed methods (questionnaires, interviews and case vignettes after completion of the study). The feasibility of the study was assessed concerning success of achieving recruitment targets, balancing cluster sizes and minimising drop-out rates. Exploratory outcomes included the medication appropriateness index (MAI), quality of life, functional status and adherence-related measures. MAI was evaluated blinded to group assignment, and intra-rater/inter-rater reliability was assessed for a subsample of prescriptions.
Results: 10 practices were randomised and analysed per group. GPs/HCAs were satisfied with the interventions despite the time required (35/45 min/patient). In case vignettes, GPs/HCAs needed help using the CDSS. The study made no patients feel uneasy. Intra-rater/inter-rater reliability for MAI was excellent. Inclusion criteria were challenging and potentially inadequate, and should therefore be adjusted. Outcome measures on pain, functionality and self-reported adherence were unfeasible due to frequent missing values, an incorrect manual or potentially invalid results.
Conclusions: Intervention and trial design were feasible. The pilot study revealed important limitations that influenced the design and conduct of the main study, thus highlighting the value of piloting complex interventions.
Trial registration number: ISRCTN99691973; Results.
Keywords: Multimorbidity; comorbidity; complex intervention; drug therapy, computer-assisted; medication adherence; polypharmacy.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical