

Effect of Radiosurgery Alone vs Radiosurgery With Whole Brain Radiation Therapy on Cognitive Function in Patients With 1 to 3 Brain Metastases: A Randomized Clinical Trial
- PMID: 27458945
- PMCID: PMC5313044
- DOI: 10.1001/jama.2016.9839
Effect of Radiosurgery Alone vs Radiosurgery With Whole Brain Radiation Therapy on Cognitive Function in Patients With 1 to 3 Brain Metastases: A Randomized Clinical Trial
Erratum in
-
Incorrect Data.JAMA. 2018 Aug 7;320(5):510. doi: 10.1001/jama.2018.9890. JAMA. 2018. PMID: 30087988 Free PMC article. No abstract available.
Abstract
Importance: Whole brain radiotherapy (WBRT) significantly improves tumor control in the brain after stereotactic radiosurgery (SRS), yet because of its association with cognitive decline, its role in the treatment of patients with brain metastases remains controversial.
Objective: To determine whether there is less cognitive deterioration at 3 months after SRS alone vs SRS plus WBRT.
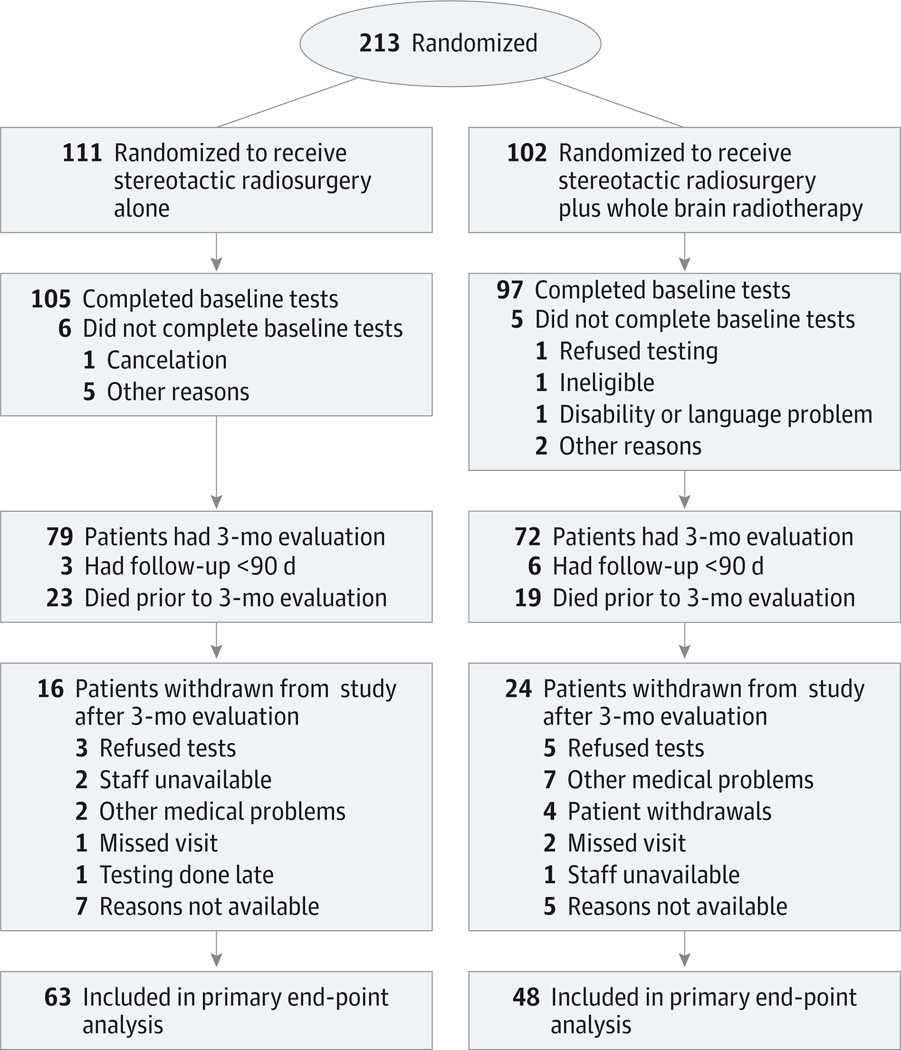
Design, setting, and participants: At 34 institutions in North America, patients with 1 to 3 brain metastases were randomized to receive SRS or SRS plus WBRT between February 2002 and December 2013.
Interventions: The WBRT dose schedule was 30 Gy in 12 fractions; the SRS dose was 18 to 22 Gy in the SRS plus WBRT group and 20 to 24 Gy for SRS alone.
Main outcomes and measures: The primary end point was cognitive deterioration (decline >1 SD from baseline on at least 1 cognitive test at 3 months) in participants who completed the baseline and 3-month assessments. Secondary end points included time to intracranial failure, quality of life, functional independence, long-term cognitive status, and overall survival.
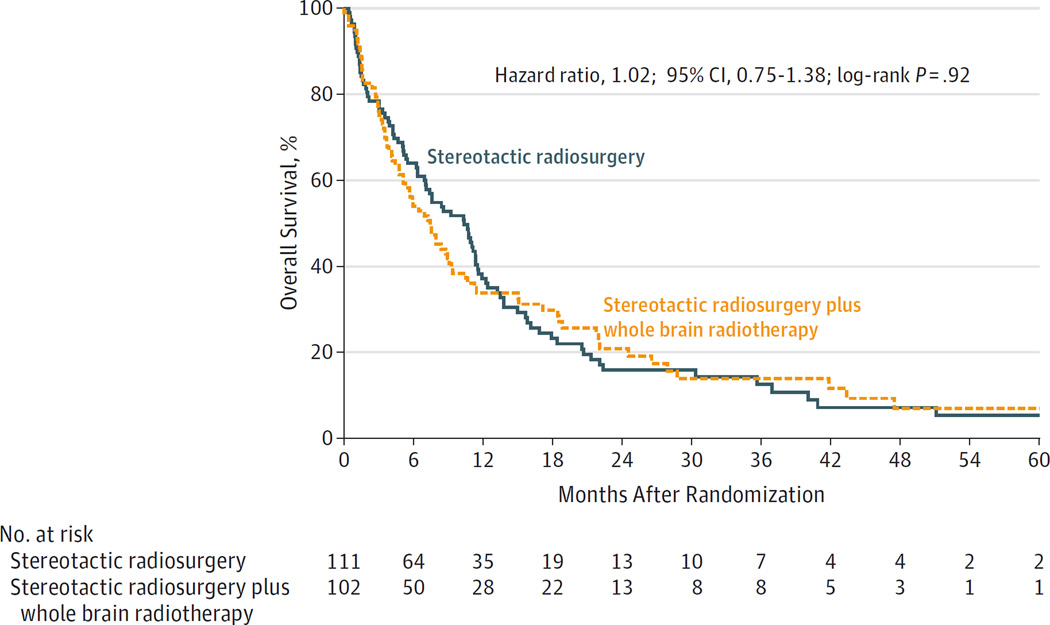
Results: There were 213 randomized participants (SRS alone, n = 111; SRS plus WBRT, n = 102) with a mean age of 60.6 years (SD, 10.5 years); 103 (48%) were women. There was less cognitive deterioration at 3 months after SRS alone (40/63 patients [63.5%]) than when combined with WBRT (44/48 patients [91.7%]; difference, -28.2%; 90% CI, -41.9% to -14.4%; P < .001). Quality of life was higher at 3 months with SRS alone, including overall quality of life (mean change from baseline, -0.1 vs -12.0 points; mean difference, 11.9; 95% CI, 4.8-19.0 points; P = .001). Time to intracranial failure was significantly shorter for SRS alone compared with SRS plus WBRT (hazard ratio, 3.6; 95% CI, 2.2-5.9; P < .001). There was no significant difference in functional independence at 3 months between the treatment groups (mean change from baseline, -1.5 points for SRS alone vs -4.2 points for SRS plus WBRT; mean difference, 2.7 points; 95% CI, -2.0 to 7.4 points; P = .26). Median overall survival was 10.4 months for SRS alone and 7.4 months for SRS plus WBRT (hazard ratio, 1.02; 95% CI, 0.75-1.38; P = .92). For long-term survivors, the incidence of cognitive deterioration was less after SRS alone at 3 months (5/11 [45.5%] vs 16/17 [94.1%]; difference, -48.7%; 95% CI, -87.6% to -9.7%; P = .007) and at 12 months (6/10 [60%] vs 17/18 [94.4%]; difference, -34.4%; 95% CI, -74.4% to 5.5%; P = .04).
Conclusions and relevance: Among patients with 1 to 3 brain metastases, the use of SRS alone, compared with SRS combined with WBRT, resulted in less cognitive deterioration at 3 months. In the absence of a difference in overall survival, these findings suggest that for patients with 1 to 3 brain metastases amenable to radiosurgery, SRS alone may be a preferred strategy.
Trial registration: clinicaltrials.gov Identifier: NCT00377156.
Conflict of interest statement
Figures

Comment in
-
Whole Brain Radiotherapy for Brain Metastases: Is the Debate Over?JAMA. 2016 Jul 26;316(4):393-5. doi: 10.1001/jama.2016.8692. JAMA. 2016. PMID: 27458941 No abstract available.
-
Effect of Whole Brain Radiation Therapy on Cognitive Function.Neurosurgery. 2017 Mar 1;80(3):N7-N16. doi: 10.1093/neuros/nyw121. Neurosurgery. 2017. PMID: 28362974 No abstract available.
References
-
- Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. JAMA. 2006;295(21):2483–2491. - PubMed
-
- Nabors LB, Portnow J, Ammirati M, et al. Central nervous system cancers, version 1.2015. J Natl Compr Canc Netw. 2015;13(10):1191–1202. - PubMed
-
- Chang EL, Wefel JS, Hess KR, et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: a randomised controlled trial. Lancet Oncol. 2009;10(11):1037–1044. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U10 CA180868/CA/NCI NIH HHS/United States
- CA076001/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- U10CA180882/CA/NCI NIH HHS/United States
- UG1 CA189823/CA/NCI NIH HHS/United States
- U10 CA180882/CA/NCI NIH HHS/United States
- U10 CA021661/CA/NCI NIH HHS/United States
- U10 CA076001/CA/NCI NIH HHS/United States
- CA025224/CA/NCI NIH HHS/United States
- U10CA180868/CA/NCI NIH HHS/United States
- U10CA180821/CA/NCI NIH HHS/United States
- U10 CA180867/CA/NCI NIH HHS/United States
- U10 CA025224/CA/NCI NIH HHS/United States
- U10CA21661/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
