

The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The Hypothesis of PCOS as Functional Ovarian Hyperandrogenism Revisited
- PMID: 27459230
- PMCID: PMC5045492
- DOI: 10.1210/er.2015-1104
The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The Hypothesis of PCOS as Functional Ovarian Hyperandrogenism Revisited
Abstract
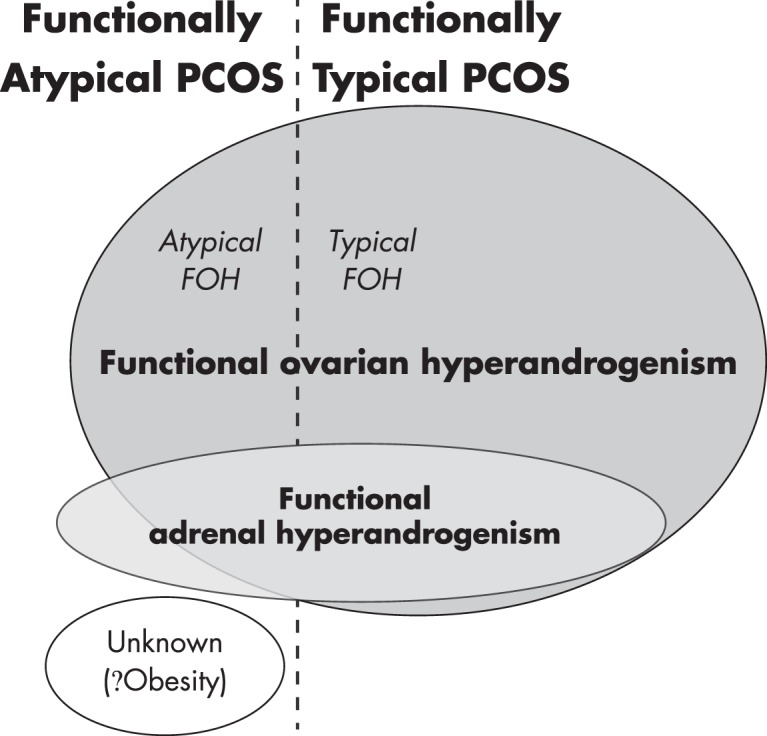
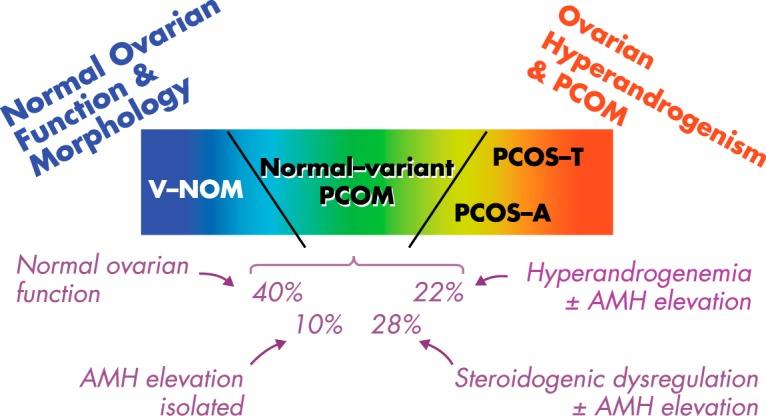
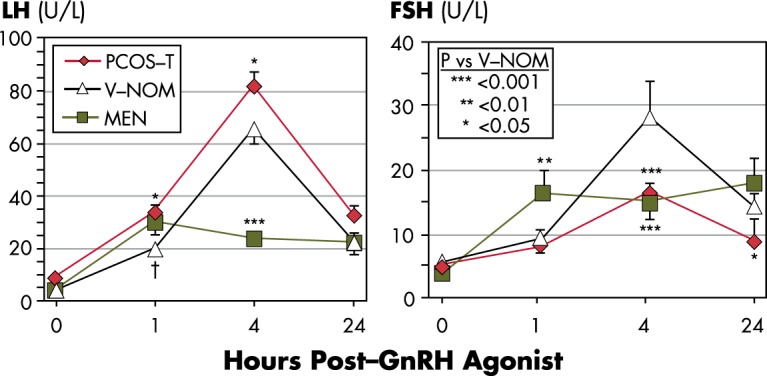
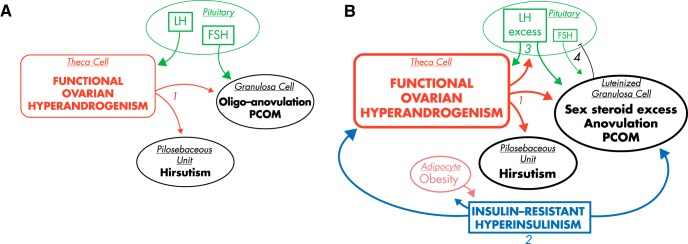
Polycystic ovary syndrome (PCOS) was hypothesized to result from functional ovarian hyperandrogenism (FOH) due to dysregulation of androgen secretion in 1989-1995. Subsequent studies have supported and amplified this hypothesis. When defined as otherwise unexplained hyperandrogenic oligoanovulation, two-thirds of PCOS cases have functionally typical FOH, characterized by 17-hydroxyprogesterone hyperresponsiveness to gonadotropin stimulation. Two-thirds of the remaining PCOS have FOH detectable by testosterone elevation after suppression of adrenal androgen production. About 3% of PCOS have a related isolated functional adrenal hyperandrogenism. The remaining PCOS cases are mild and lack evidence of steroid secretory abnormalities; most of these are obese, which we postulate to account for their atypical PCOS. Approximately half of normal women with polycystic ovarian morphology (PCOM) have subclinical FOH-related steroidogenic defects. Theca cells from polycystic ovaries of classic PCOS patients in long-term culture have an intrinsic steroidogenic dysregulation that can account for the steroidogenic abnormalities typical of FOH. These cells overexpress most steroidogenic enzymes, particularly cytochrome P450c17. Overexpression of a protein identified by genome-wide association screening, differentially expressed in normal and neoplastic development 1A.V2, in normal theca cells has reproduced this PCOS phenotype in vitro. A metabolic syndrome of obesity-related and/or intrinsic insulin resistance occurs in about half of PCOS patients, and the compensatory hyperinsulinism has tissue-selective effects, which include aggravation of hyperandrogenism. PCOS seems to arise as a complex trait that results from the interaction of diverse genetic and environmental factors. Heritable factors include PCOM, hyperandrogenemia, insulin resistance, and insulin secretory defects. Environmental factors include prenatal androgen exposure and poor fetal growth, whereas acquired obesity is a major postnatal factor. The variety of pathways involved and lack of a common thread attests to the multifactorial nature and heterogeneity of the syndrome. Further research into the fundamental basis of the disorder will be necessary to optimally correct androgen levels, ovulation, and metabolic homeostasis.
Figures
References
-
- Ehrmann DA. Polycystic ovary syndrome. N Engl J Med. 2005;352:1223–1236. - PubMed
-
- Lauritsen MP, Bentzen JG, Pinborg A, et al. The prevalence of polycystic ovary syndrome in a normal population according to the Rotterdam criteria versus revised criteria including anti-Mullerian hormone. Hum Reprod. 2014;29:791–801. - PubMed
-
- Stein IF, Leventhal ML. Amenorrhea associated with bilateral polycystic ovaries. Am J Obstet Gynecol. 1935;29:181–191.
-
- Azziz R, Adashi EY. Stein and Leventhal: 80 years on. Am J Obstet Gynecol. 2016;214:247.e1–247.e11. - PubMed
-
- Goldzieher MW, Green JA. The polycystic ovary. I. Clinical and histologic features. J Clin Endocrinol Metab. 1962;22:325–338. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
