

Severe hyperkalemia following adrenalectomy for aldosteronoma: prediction, pathogenesis and approach to clinical management- a case series
- PMID: 27460219
- PMCID: PMC4962422
- DOI: 10.1186/s12902-016-0121-y
Severe hyperkalemia following adrenalectomy for aldosteronoma: prediction, pathogenesis and approach to clinical management- a case series
Abstract
Background: As the field of Primary Aldosteronism (PA) becomes ever expanded, diagnosis of PA is increasingly diagnosed by endocrinologists. With increased PA screening, many of the cases are now found in patients with complex co-morbidities in addition to their hypertension. Post adrenalectomy renal impairment with hyperkalemia is now increasingly seen in these complex patients, as evidenced by the numerous reports on this issue that have appeared within the past 3 years. We present a small case series to illustrate the breadth of the problem, along with a discussion about how such CKD/hyperkalemic events may be predicted.
Case presentation: We present three cases of primary aldosteronism with long standing hypertension (more than 10 years) hypokalemia (2.0-3.0 mmol/l). Serum aldosterone was high with low renin activity leading to high aldosterone to renin ratio (ARR). They underwent abdominal CT scan revealing adrenal mass and adrenal vein sample confirmed lateralization. None of the patients had evidence of renal disease before surgery (as evident by normal eGFR and serum creatinine). Post adrenalectomy they had reduction in the blood pressure and became eukalemic. Serum aldosterone and renin activity were low leading to a low ARR. Case 1 developed hyperkalemia and increased serum creatinine 6 weeks post operatively which resolved with initiation of fludrocortisone and every attempt to discontinue fludrocortisone resulted in hyperkalemia and rising creatinine. Her hyperkalemia is under control with oral sodium bicarbonate. Case 2 developed hyperkalemia and increasing creatinine 2 months post operatively transiently requiring fludrocortisone and later on managed with furosemide for hyperkalemia. Case 3 developed renal impairment and hyperkalemia 2 weeks post operatively requiring fludrocortisone.
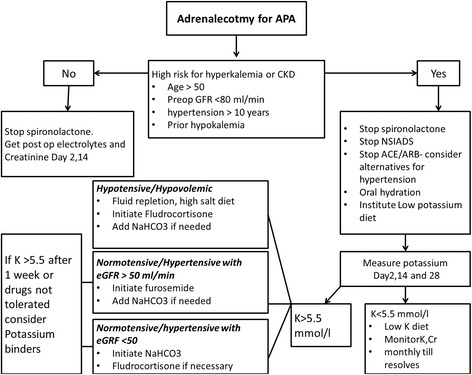
Conclusion: Post APA resection severe hyperkalemia may be a common entity and screening should be actively considered in high risk patients. Older age, longer duration of hypertension, impaired pre-op and post-op GFR and higher levels of pre-op aldosterone and are all risk factors which predict the likelihood of developing post-operative hyperkalemia. Fludrocortisone, sodium bicarbonate, loop diuretics and potassium binders can be used for treatment. Treatment choice should be tailored to patient characteristics including fluid status, blood pressure and serum creatinine. Potassium binders should be avoided in patients with history of recent abdominal surgery, opioid use and constipation. Serum electrolytes and creatinine should be monitored every 1-2 weeks after starting treatment to ensure an adequate response. Prolonged management may be necessary in some cases and at-risk patients should be counselled as to the meaning and importance of post-operative changes in measured renal function and potassium.
Keywords: Adrenalectomy; Aldosteronoma; Case report; Hyperkalemia.
Figures
Similar articles
-
[Persistent and serious hyperkalemia after surgery of primary aldosteronism: A case report].Beijing Da Xue Xue Bao Yi Xue Ban. 2022 Apr 18;54(2):376-380. doi: 10.19723/j.issn.1671-167X.2022.02.028. Beijing Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35435207 Free PMC article. Review. Chinese.
-
Contralateral suppression of aldosterone at adrenal venous sampling predicts hyperkalemia following adrenalectomy for primary aldosteronism.Surgery. 2018 Jan;163(1):183-190. doi: 10.1016/j.surg.2017.07.034. Epub 2017 Nov 9. Surgery. 2018. PMID: 29129366
-
Insufficiency of the zona glomerulosa of the adrenal cortex and progressive kidney insufficiency following unilateral adrenalectomy - case report and discussion.Blood Press. 2018 Oct;27(5):304-312. doi: 10.1080/08037051.2018.1470460. Epub 2018 May 9. Blood Press. 2018. PMID: 29742971
-
Incidence and factors of post-adrenalectomy hyperkalemia in patients with aldosterone producing adenoma.Clin Chim Acta. 2013 Sep 23;424:114-8. doi: 10.1016/j.cca.2013.05.017. Epub 2013 May 28. Clin Chim Acta. 2013. PMID: 23727469
-
Severe hydronephrosis complicated with primary aldosteronism: a case report and review of the literature.J Med Case Rep. 2024 Oct 6;18(1):463. doi: 10.1186/s13256-024-04798-4. J Med Case Rep. 2024. PMID: 39369228 Free PMC article. Review.
Cited by
-
Persistent severe hyperkalemia following surgical treatment of aldosterone-producing adenoma.J Res Med Sci. 2020 Feb 20;25:17. doi: 10.4103/jrms.JRMS_603_19. eCollection 2020. J Res Med Sci. 2020. PMID: 32174989 Free PMC article.
-
Contralateral Suppression at Adrenal Venous Sampling Is Associated with Renal Impairment Following Adrenalectomy for Unilateral Primary Aldosteronism.Endocrinol Metab (Seoul). 2021 Aug;36(4):875-884. doi: 10.3803/EnM.2021.1047. Epub 2021 Aug 11. Endocrinol Metab (Seoul). 2021. PMID: 34376041 Free PMC article.
-
Cerebro-Cardiovascular Risk, Target Organ Damage, and Treatment Outcomes in Primary Aldosteronism.Front Cardiovasc Med. 2022 Feb 2;8:798364. doi: 10.3389/fcvm.2021.798364. eCollection 2021. Front Cardiovasc Med. 2022. PMID: 35187110 Free PMC article. Review.
-
Adrenal Mass and Hypokalaemia: The Zebra Among Horses.Cureus. 2024 Jun 11;16(6):e62123. doi: 10.7759/cureus.62123. eCollection 2024 Jun. Cureus. 2024. PMID: 38993410 Free PMC article.
-
[Persistent and serious hyperkalemia after surgery of primary aldosteronism: A case report].Beijing Da Xue Xue Bao Yi Xue Ban. 2022 Apr 18;54(2):376-380. doi: 10.19723/j.issn.1671-167X.2022.02.028. Beijing Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35435207 Free PMC article. Review. Chinese.
References
-
- Funder JW, Carey RM, Fardella C, Gomez-Sanchez CE, Mantero F, Stowasser M, Young WF, Jr, Montori VM. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline Endocrine Society. J Clin Endocrinol Metab. 2008;93(9):3266–3281. doi: 10.1210/jc.2008-0104. - DOI - PubMed
-
- Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C, Ganzaroli C, Giacchetti G, Letizia C, Maccario M, Mallamaci F, Mannelli M, Mattarello MJ, Moretti A, Palumbo G, Parenti G, Porteri E, Semplicini A, Rizzoni D, Rossi E, Boscaro M, Pessina AC, Mantero F, PAPY Study Investigators A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006;48(11):2293–2300. doi: 10.1016/j.jacc.2006.07.059. - DOI - PubMed
-
- Fischer E, Hanslik G, Pallauf A, Degenhart C, Linsenmaier U, Beuschlein F, Bidlingmaier M, Mussack T, Ladurner R, Hallfeldt K, Quinkler M, Reincke M. Prolonged zona glomerulosa insufficiency causing hyperkalemia in primary aldosteronism after adrenalectomy. J Clin Endocrinol Metab. 2012;97(11):3965–3973. doi: 10.1210/jc.2012-2234. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
