

Body mass index: Has epidemiology started to break down causal contributions to health and disease?
- PMID: 27460712
- PMCID: PMC5972005
- DOI: 10.1002/oby.21554
Body mass index: Has epidemiology started to break down causal contributions to health and disease?
Abstract
Objectives: To review progress in understanding the methods and results concerning the causal contribution of body mass index (BMI) to health and disease.
Methods: In the context of conventional evidence focused on the relationship between BMI and health, this review considers current literature on the common, population-based, genetic contribution to BMI and how this has fed into the developing field of applied epidemiology.
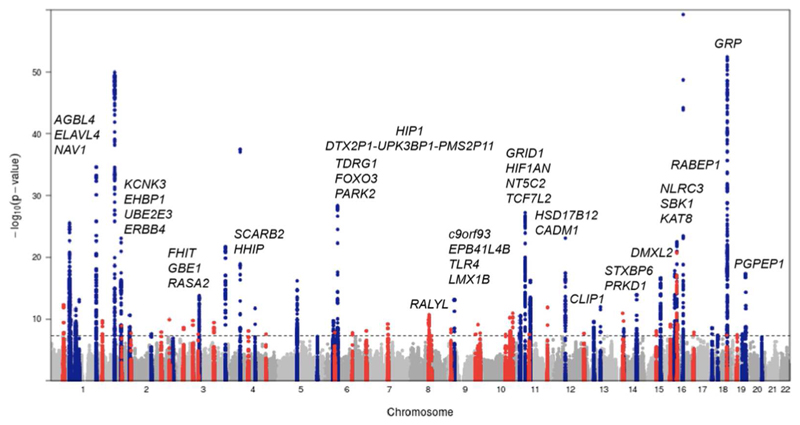
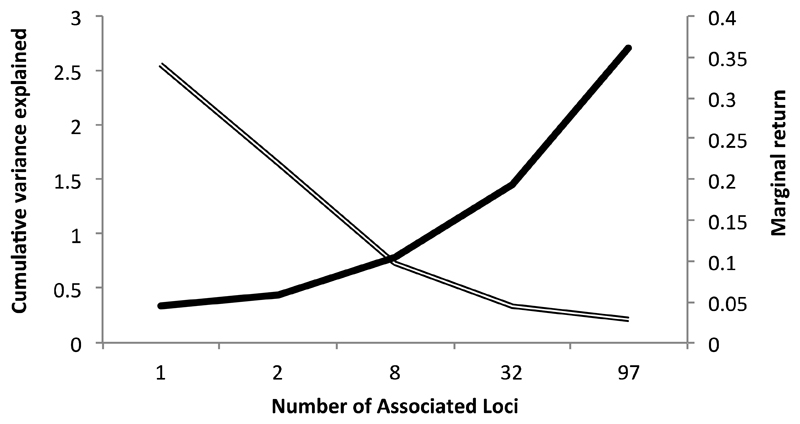
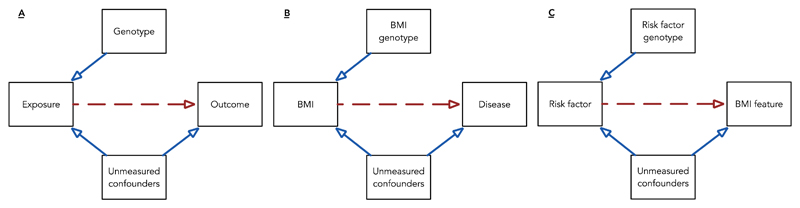
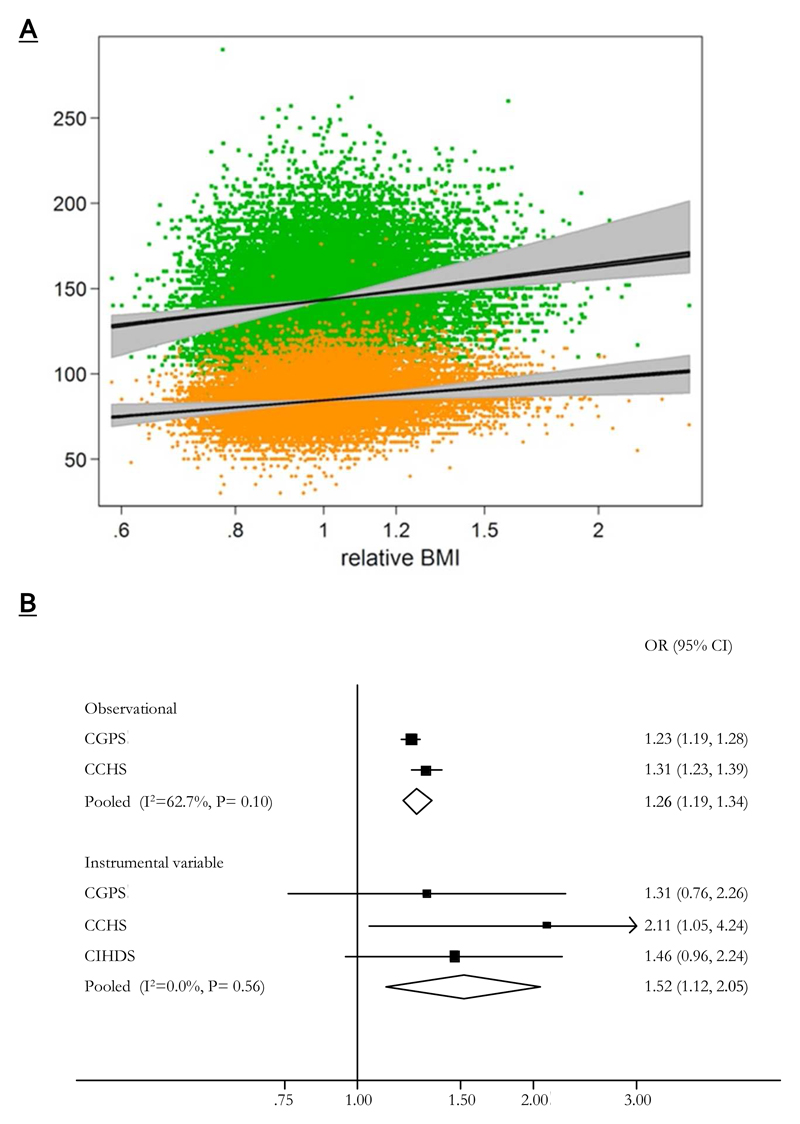
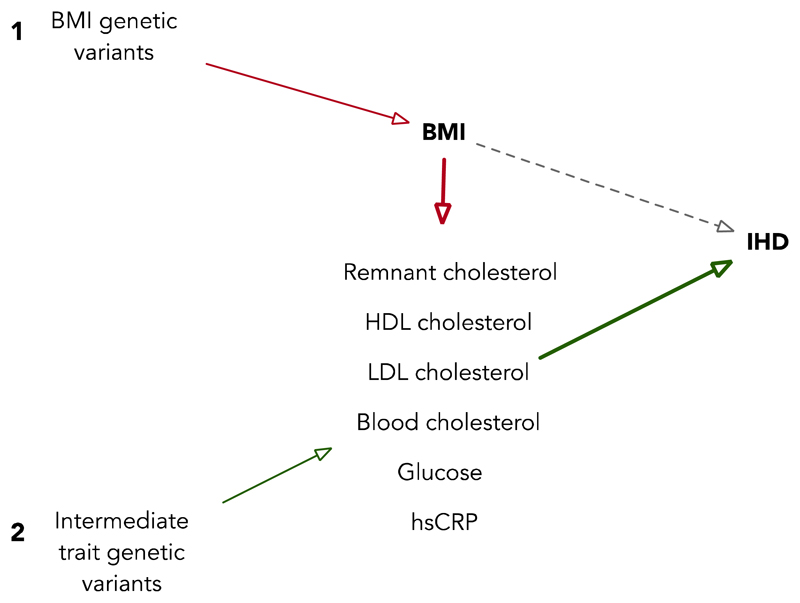
Results: Technological and analytical developments have driven considerable success in identifying genetic variants relevant to BMI. This has enabled the implementation of Mendelian randomization to address questions of causality. The product of this work has been the implication of BMI as a causal agent in a host of health outcomes. Further breakdown of causal pathways by integration with other "omics" technologies promises to deliver additional benefit.
Conclusions: Gaps remain in our understanding of BMI as a risk factor for health and disease, and while promising, applied genetic epidemiology should be considered alongside alternative methods for assessing the impact of BMI on health. Potential limitations, relating to inappropriate or nonspecific measures of obesity and the improper use of genetic instruments, will need to be explored and incorporated into future research aiming to dissect BMI as a risk factor.
© 2016 The Obesity Society.
Conflict of interest statement
Disclosure: The authors declared no conflict of interest.
Figures
References
-
- Hill JO, Peters JC. Environmental Contributions to the Obesity Epidemic. Science. 1998;280:1371–1374. - PubMed
-
- Swinburn B, Egger G, Raza F. Dissecting Obesogenic Environments: The Development and Application of a Framework for Identifying and Prioritizing Environmental Interventions for Obesity. Preventive Medicine. 1999;29:563–570. - PubMed
-
- Wolf AM, Colditz GA. Current estimates of the economic cost of obesity in the United States. Obes Res. 1998;6:97–106. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
