

Relationship Between HIV Coinfection, Interleukin 10 Production, and Mycobacterium tuberculosis in Human Lymph Node Granulomas
- PMID: 27462092
- PMCID: PMC5079364
- DOI: 10.1093/infdis/jiw313
Relationship Between HIV Coinfection, Interleukin 10 Production, and Mycobacterium tuberculosis in Human Lymph Node Granulomas
Abstract
Background: Human immunodeficiency virus type 1 (HIV)-infected persons are more susceptible to tuberculosis than HIV-uninfected persons. Low peripheral CD4+ T-cell count is not the sole cause of higher susceptibility, because HIV-infected persons with a high peripheral CD4+ T-cell count and those prescribed successful antiretroviral therapy (ART) remain more prone to active tuberculosis than HIV-uninfected persons. We hypothesized that the increase in susceptibility is caused by the ability of HIV to manipulate Mycobacterium tuberculosis-associated granulomas.
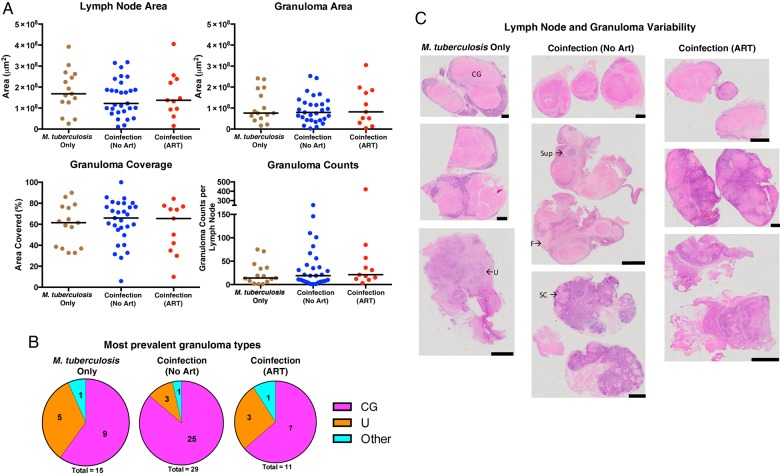
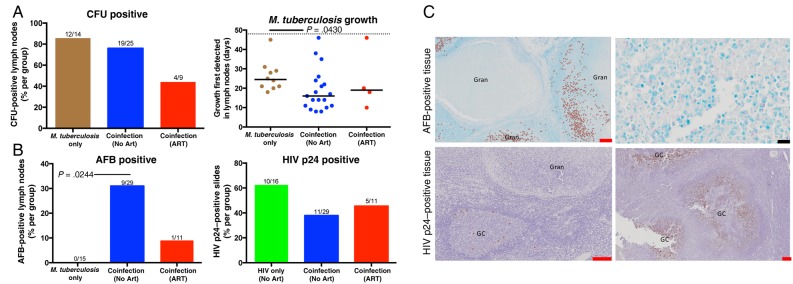
Methods: We examined 71 excised cervical lymph nodes (LNs) from persons with HIV and M. tuberculosis coinfection, those with HIV monoinfection, and those with M. tuberculosis monoinfection with a spectrum of peripheral CD4+ T-cell counts and ART statuses. We quantified differences in M. tuberculosis levels, HIV p24 levels, cellular response, and cytokine presence within granulomas.
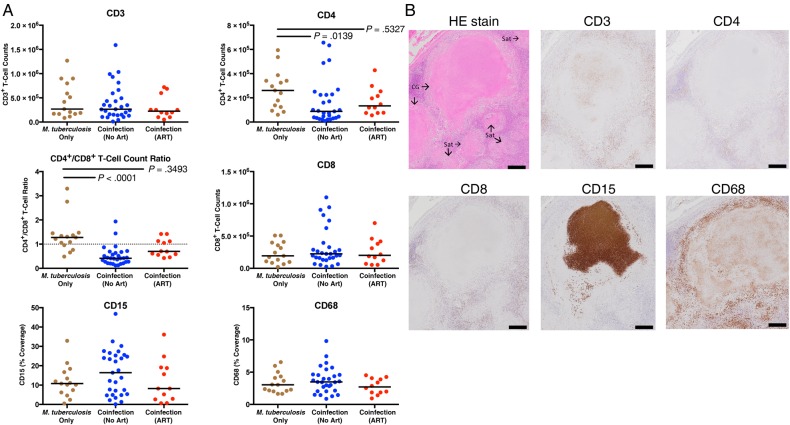
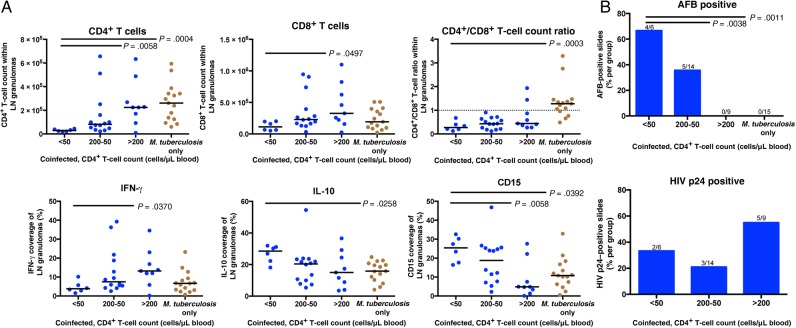
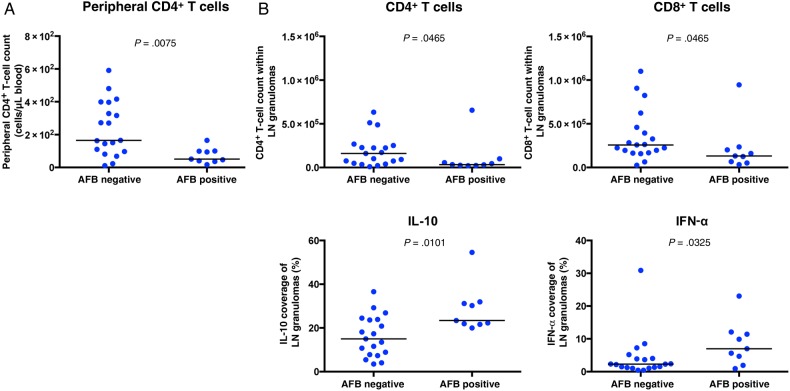
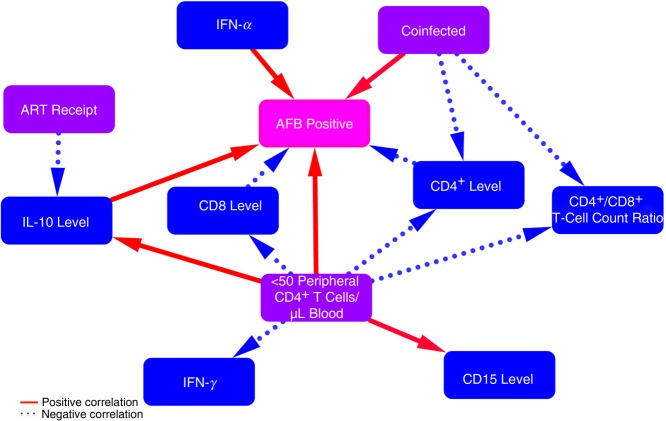
Results: HIV increased M. tuberculosis numbers and reduced CD4+ T-cell counts within granulomas. Peripheral CD4+ T-cell depletion correlated with granulomas that contained fewer CD4+ and CD8+ T cells, less interferon γ, more neutrophils, more interleukin 10 (IL-10), and increased M. tuberculosis numbers. M. tuberculosis numbers correlated positively with IL-10 and interferon α levels and fewer CD4+ and CD8+ T cells. ART reduced IL-10 production.
Conclusions: Peripheral CD4+ T-cell depletion correlated with increased M. tuberculosis presence, increased IL-10 production, and other phenotypic changes within granulomas, demonstrating the HIV infection progressively changes these granulomas.
Keywords: HIV; IL-10; antiretroviral therapy; coinfection; granuloma; histology; lymph node; mycobacterium; tuberculosis.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures

Comment in
-
Granulomatous Responses in HIV and Mycobacterium tuberculosis Coinfection.J Infect Dis. 2016 Nov 1;214(9):1292-1293. doi: 10.1093/infdis/jiw314. Epub 2016 Jul 26. J Infect Dis. 2016. PMID: 27462091 No abstract available.
Similar articles
-
The Pathology of Lymphocytes, Histiocytes, and Immune Mechanisms in Mycobacterium tuberculosis Granulomas.Am J Trop Med Hyg. 2021 Mar 15;104(5):1796-1802. doi: 10.4269/ajtmh.20-1372. Am J Trop Med Hyg. 2021. PMID: 33720848 Free PMC article.
-
Hierarchy Low CD4+/CD8+ T-Cell Counts and IFN-γ Responses in HIV-1+ Individuals Correlate with Active TB and/or M.tb Co-Infection.PLoS One. 2016 Mar 9;11(3):e0150941. doi: 10.1371/journal.pone.0150941. eCollection 2016. PLoS One. 2016. PMID: 26959228 Free PMC article.
-
HIV-1 Infection Is Associated with Depletion and Functional Impairment of Mycobacterium tuberculosis-Specific CD4 T Cells in Individuals with Latent Tuberculosis Infection.J Immunol. 2017 Sep 15;199(6):2069-2080. doi: 10.4049/jimmunol.1700558. Epub 2017 Jul 31. J Immunol. 2017. PMID: 28760884 Free PMC article.
-
Interaction between HIV and Mycobacterium tuberculosis: HIV-1-induced CD4 T-cell depletion and the development of active tuberculosis.Curr Opin HIV AIDS. 2012 May;7(3):268-75. doi: 10.1097/COH.0b013e3283524e32. Curr Opin HIV AIDS. 2012. PMID: 22495739 Review.
-
Recent progress in understanding immune activation in the pathogenesis in HIV-tuberculosis co-infection.Curr Opin HIV AIDS. 2018 Nov;13(6):455-461. doi: 10.1097/COH.0000000000000501. Curr Opin HIV AIDS. 2018. PMID: 30286038 Review.
Cited by
-
Role of Type I Interferons during Mycobacterium tuberculosis and HIV Infections.Biomolecules. 2024 Jul 14;14(7):848. doi: 10.3390/biom14070848. Biomolecules. 2024. PMID: 39062562 Free PMC article. Review.
-
A non-canonical type 2 immune response coordinates tuberculous granuloma formation and epithelialization.Cell. 2021 Apr 1;184(7):1757-1774.e14. doi: 10.1016/j.cell.2021.02.046. Epub 2021 Mar 23. Cell. 2021. PMID: 33761328 Free PMC article.
-
Spontaneous Control of SIV Replication Does Not Prevent T Cell Dysregulation and Bacterial Dissemination in Animals Co-Infected with M. tuberculosis.Microbiol Spectr. 2022 Jun 29;10(3):e0172421. doi: 10.1128/spectrum.01724-21. Epub 2022 Apr 25. Microbiol Spectr. 2022. PMID: 35467372 Free PMC article.
-
Single Cell Analysis of Peripheral TB-Associated Granulomatous Lymphadenitis.bioRxiv [Preprint]. 2024 Jun 26:2024.05.28.596301. doi: 10.1101/2024.05.28.596301. bioRxiv. 2024. PMID: 38853908 Free PMC article. Preprint.
-
HIV-MTB Co-Infection Reduces CD4+ T Cells and Affects Granuloma Integrity.Viruses. 2024 Aug 21;16(8):1335. doi: 10.3390/v16081335. Viruses. 2024. PMID: 39205309 Free PMC article.
References
-
- World Health Organization. Global tuberculosis report 2014. Geneva: World Health Organization, 2015.
-
- World Health Organization. Consolidated strategic information guidelines for HIV in the health sector. Geneva: World Health Organization, 2015. - PubMed
-
- Caruso AM, Serbina N, Klein E, Triebold K, Bloom BR, Flynn JL. Mice deficient in CD4 T cells have only transiently diminished levels of IFN-gamma, yet succumb to tuberculosis. J Immunol 1999; 162:5407–16. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
