

Umbilical hernia in patients with liver cirrhosis: A surgical challenge
- PMID: 27462389
- PMCID: PMC4942747
- DOI: 10.4240/wjgs.v8.i7.476
Umbilical hernia in patients with liver cirrhosis: A surgical challenge
Abstract
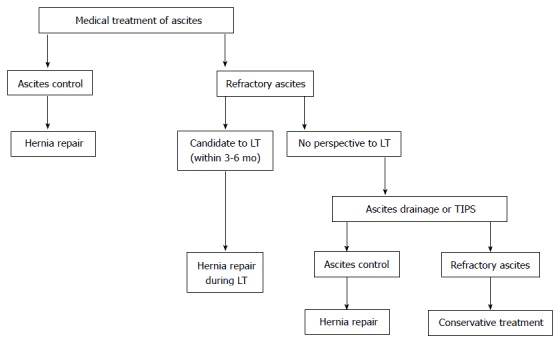
Umbilical hernia occurs in 20% of the patients with liver cirrhosis complicated with ascites. Due to the enormous intraabdominal pressure secondary to the ascites, umbilical hernia in these patients has a tendency to enlarge rapidly and to complicate. The treatment of umbilical hernia in these patients is a surgical challenge. Ascites control is the mainstay to reduce hernia recurrence and postoperative complications, such as wound infection, evisceration, ascites drainage, and peritonitis. Intermittent paracentesis, temporary peritoneal dialysis catheter or transjugular intrahepatic portosystemic shunt may be necessary to control ascites. Hernia repair is indicated in patients in whom medical treatment is effective in controlling ascites. Patients who have a good perspective to be transplanted within 3-6 mo, herniorrhaphy should be performed during transplantation. Hernia repair with mesh is associated with lower recurrence rate, but with higher surgical site infection when compared to hernia correction with conventional fascial suture. There is no consensus on the best abdominal wall layer in which the mesh should be placed: Onlay, sublay, or underlay. Many studies have demonstrated several advantages of the laparoscopic umbilical herniorrhaphy in cirrhotic patients compared with open surgical treatment.
Keywords: Ascites; Ascites drainage; Hernia repair; Liver cirrhosis; Liver transplantation; Mesh; Surgical site infection; Umbilical hernia.
Figures
References
-
- Cassie S, Okrainec A, Saleh F, Quereshy FS, Jackson TD. Laparoscopic versus open elective repair of primary umbilical hernias: short-term outcomes from the American College of Surgeons National Surgery Quality Improvement Program. Surg Endosc. 2014;28:741–746. - PubMed
-
- Sarit C, Eliezer A, Mizrahi S. Minimally invasive repair of recurrent strangulated umbilical hernia in cirrhotic patient with refractory ascites. Liver Transpl. 2003;9:621–622. - PubMed
-
- Ammar SA. Management of complicated umbilical hernias in cirrhotic patients using permanent mesh: randomized clinical trial. Hernia. 2010;14:35–38. - PubMed
-
- Carbonell AM, Wolfe LG, DeMaria EJ. Poor outcomes in cirrhosis-associated hernia repair: a nationwide cohort study of 32,033 patients. Hernia. 2005;9:353–357. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
