

Deep-Plane Lipoabdominoplasty in East Asians
- PMID: 27462568
- PMCID: PMC4959978
- DOI: 10.5999/aps.2016.43.4.352
Deep-Plane Lipoabdominoplasty in East Asians
Abstract
Background: The objective of this study was to develop a new surgical technique by combining traditional abdominoplasty with liposuction. This combination of operations permits simpler and more accurate management of various abdominal deformities. In lipoabdominoplasty, the combination of techniques is of paramount concern. Herein, we introduce a new combination of liposuction and abdominoplasty using deep-plane flap sliding to maximize the benefits of both techniques.
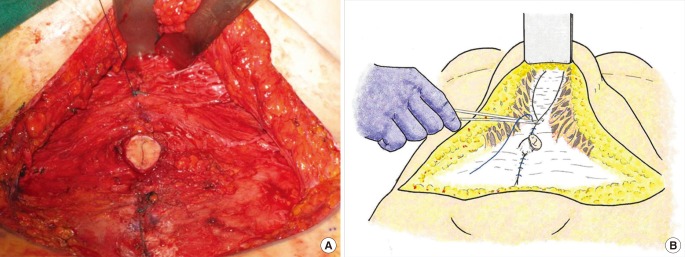
Methods: Deep-plane lipoabdominoplasty was performed in 143 patients between January 2007 and May 2014. We applied extensive liposuction on the entire abdomen followed by a sliding flap through the deep plane after repairing the diastasis recti. The abdominal wound closure was completed with repair of Scarpa's fascia.
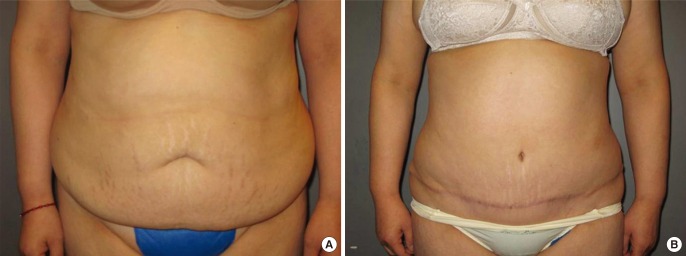
Results: The average amount of liposuction aspirate was 1,400 mL (700-3,100 mL), and the size of the average excised skin ellipse was 21.78×12.81 cm (from 15×10 to 25×15 cm). There were no major complications such as deep-vein thrombosis or pulmonary embolism. We encountered 22 cases of minor complications: one wound infection, one case of skin necrosis, two cases of undercorrection, nine hypertrophic scars, and nine seromas. These complications were solved by conservative management or simple revision.
Conclusions: The use of deep-plane lipoabdominoplasty can correct abdominal deformities more effectively and with fewer complications than traditional abdominoplasty.
Keywords: Abdominal wound closure techniques; Abdominoplasty; Lipectomy.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures







Similar articles
-
Sub-Scarpa's Lipectomy in Abdominoplasty: An Analysis of Risks and Rewards in 723 Consecutive Patients.Aesthet Surg J. 2019 Aug 22;39(9):966-976. doi: 10.1093/asj/sjz027. Aesthet Surg J. 2019. PMID: 30722005
-
Prospective clinical study of 551 cases of liposuction and abdominoplasty performed individually and in combination.Plast Reconstr Surg Glob Open. 2013 Sep 10;1(5):e32. doi: 10.1097/GOX.0b013e3182a333d7. eCollection 2013 Aug. Plast Reconstr Surg Glob Open. 2013. PMID: 25289226 Free PMC article.
-
Complication rates of lipoabdominoplasty versus traditional abdominoplasty in high-risk patients.Plast Reconstr Surg. 2010 Feb;125(2):683-690. doi: 10.1097/PRS.0b013e3181c82fb0. Plast Reconstr Surg. 2010. PMID: 20124853
-
Safety of Lipoabdominoplasty Versus Abdominoplasty: A Systematic Review and Meta-analysis.Aesthetic Plast Surg. 2019 Feb;43(1):167-174. doi: 10.1007/s00266-018-1270-3. Epub 2018 Dec 3. Aesthetic Plast Surg. 2019. PMID: 30511162
-
Lipoabdominoplasty with Anatomical Definition: Update.Clin Plast Surg. 2024 Jan;51(1):45-57. doi: 10.1016/j.cps.2023.06.011. Epub 2023 Aug 20. Clin Plast Surg. 2024. PMID: 37945075 Review.
Cited by
-
Correcting Flank Skin Laxity and Dog Ear Plus Aggressive Liposuction: A Technique for Classic Abdominoplasty in Middle-Eastern Obese Women.World J Plast Surg. 2018 Jan;7(1):78-88. World J Plast Surg. 2018. PMID: 29651396 Free PMC article.
-
Treatment Options for Abdominal Rectus Diastasis.Front Surg. 2019 Nov 19;6:65. doi: 10.3389/fsurg.2019.00065. eCollection 2019. Front Surg. 2019. PMID: 31803753 Free PMC article. Review.
-
[Research progress of abdominoplasty].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018 Dec 15;32(12):1611-1614. doi: 10.7507/1002-1892.201805088. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2018. PMID: 30569692 Free PMC article. Review. Chinese.
References
-
- Stuerz K, Piza H, Kinzl JF. The impact of abdominoplasty after massive weight loss: a qualitative study. Ann Plast Surg. 2013;71:547–549. - PubMed
-
- Stewart KJ, Stewart DA, Coghlan B, et al. Complications of 278 consecutive abdominoplasties. J Plast Reconstr Aesthet Surg. 2006;59:1152–1155. - PubMed
-
- Saldanha OR, De Souza Pinto EB, Mattos WN, Jr, et al. Lipoabdominoplasty with selective and safe undermining. Aesthetic Plast Surg. 2003;27:322–327. - PubMed
-
- Anuurad E, Shiwaku K, Nogi A, et al. The new BMI criteria for asians by the regional office for the western pacific region of WHO are suitable for screening of overweight to prevent metabolic syndrome in elder Japanese workers. J Occup Health. 2003;45:335–343. - PubMed
-
- Vernon S. Umbilical transplantation upward and abdominal contouring in lipectomy. Am J Surg. 1957;94:490–492. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources