

A pancreatic ductal adenocarcinoma subpopulation is sensitive to FK866, an inhibitor of NAMPT
- PMID: 27462772
- PMCID: PMC5288221
- DOI: 10.18632/oncotarget.10776
A pancreatic ductal adenocarcinoma subpopulation is sensitive to FK866, an inhibitor of NAMPT
Abstract
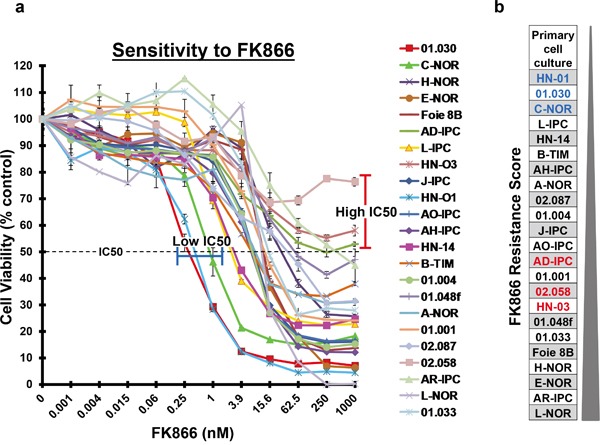
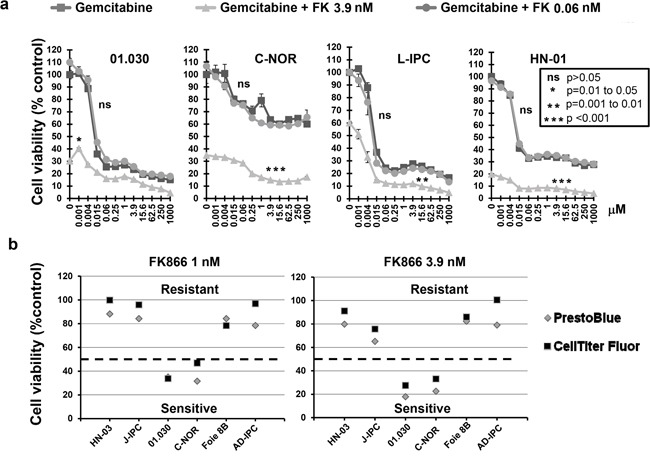
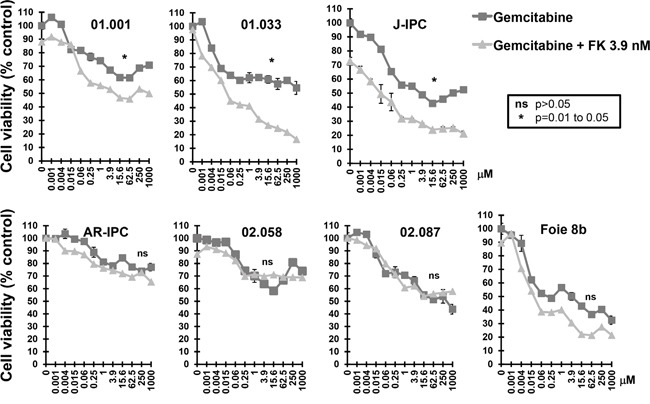
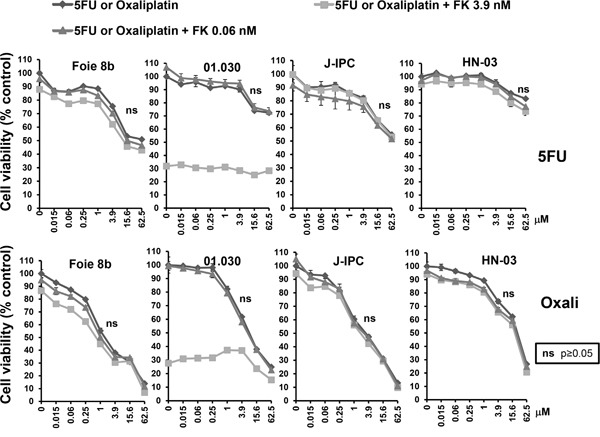
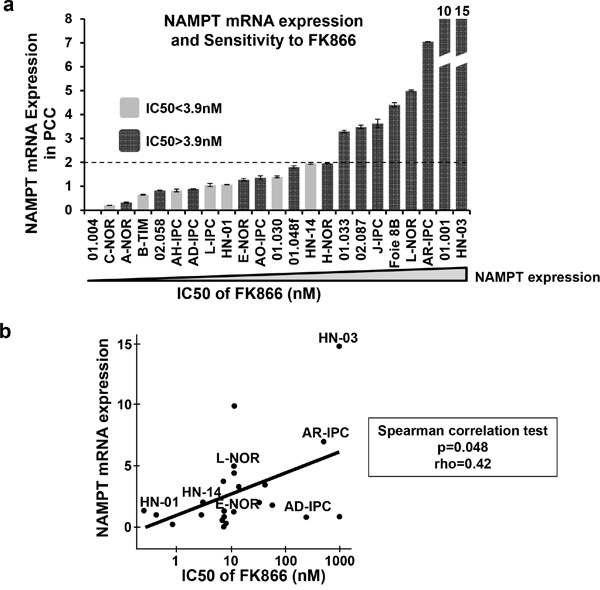
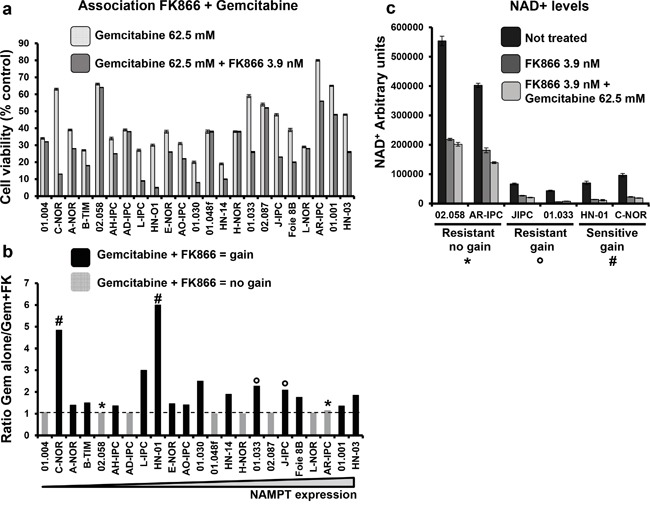
Treating pancreatic cancer is extremely challenging due to multiple factors, including chemoresistance and poor disease prognosis. Chemoresistance can be explained by: the presence of a dense stromal barrier leading to a lower vascularized condition, therefore limiting drug delivery; the huge intra-tumoral heterogeneity; and the status of epithelial-to-mesenchymal transition. These factors are highly variable between patients making it difficult to predict responses to chemotherapy. Nicotinamide phosphoribosyl transferase (NAMPT) is the main enzyme responsible for recycling cytosolic NAD+ in hypoxic conditions. FK866 is a noncompetitive specific inhibitor of NAMPT, which has proven anti-tumoral effects, although a clinical advantage has still not been demonstrated. Here, we tested the effect of FK866 on pancreatic cancer-derived primary cell cultures (PCCs), both alone and in combination with three different drugs typically used against this cancer: gemcitabine, 5-Fluorouracil (5FU) and oxaliplatin. The aims of this study were to evaluate the benefit of drug combinations, define groups of sensitivity, and identify a potential biomarker for predicting treatment sensitivity. We performed cell viability tests in the presence of either FK866 alone or in combination with the drugs above-mentioned. We confirmed both inter- and intra-tumoral heterogeneity. Interestingly, only the in vitro effect of gemcitabine was influenced by the addition of FK866. We also found that NAMPT mRNA expression levels can predict the sensitivity of cells to FK866. Overall, our results suggest that patients with tumors sensitive to FK866 can be identified using NAMPT mRNA levels as a biomarker and could therefore benefit from a co-treatment of gemcitabine plus FK866.
Keywords: FK866; NAMPT; chemotherapy; pancreatic cancer.
Conflict of interest statement
The authors disclose no conflicts of interest.
Figures
References
-
- Neesse A, Michl P, Frese KK, Feig C, Cook N, Jacobetz MA, Lolkema MP, Buchholz M, Olive KP, Gress TM, Tuveson DA. Stromal biology and therapy in pancreatic cancer. Gut. 2011;60:861–868. - PubMed
-
- Samuel N, Hudson TJ. The molecular and cellular heterogeneity of pancreatic ductal adenocarcinoma. Nature reviews Gastroenterology & hepatology. 2012;9:77–87. - PubMed
-
- Guillaumond F, Leca J, Olivares O, Lavaut MN, Vidal N, Berthezene P, Dusetti NJ, Loncle C, Calvo E, Turrini O, Iovanna JL, Tomasini R, Vasseur S. Strengthened glycolysis under hypoxia supports tumor symbiosis and hexosamine biosynthesis in pancreatic adenocarcinoma. Proceedings of the National Academy of Sciences of the United States of America. 2013;110:3919–3924. - PMC - PubMed
-
- Warburg O. On the origin of cancer cells. Science. 1956;123:309–314. - PubMed
-
- Chiarugi A, Dolle C, Felici R, Ziegler M. The NAD metabolome–a key determinant of cancer cell biology. Nature reviews Cancer. 2012;12:741–752. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
