

Old age at diagnosis increases risk of tumor progression in nasopharyngeal cancer
- PMID: 27463012
- PMCID: PMC5323224
- DOI: 10.18632/oncotarget.10818
Old age at diagnosis increases risk of tumor progression in nasopharyngeal cancer
Abstract
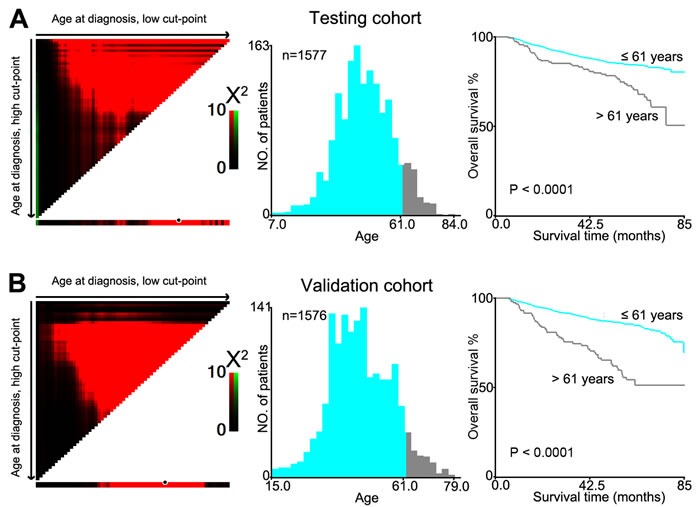
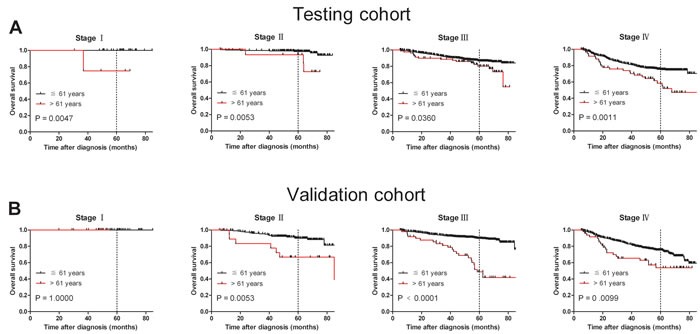
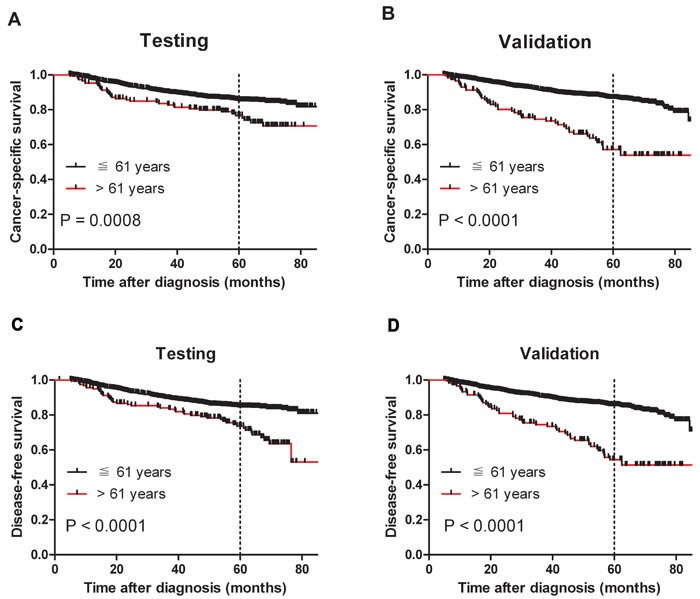
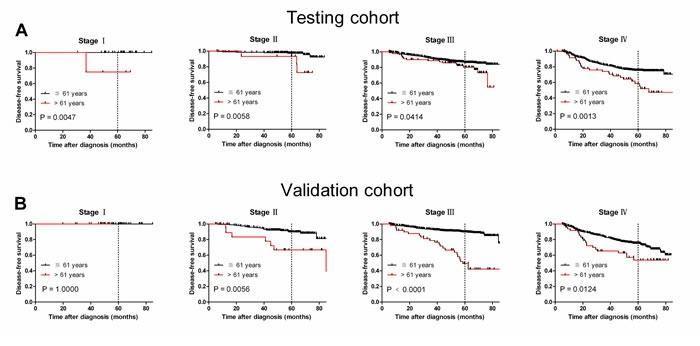
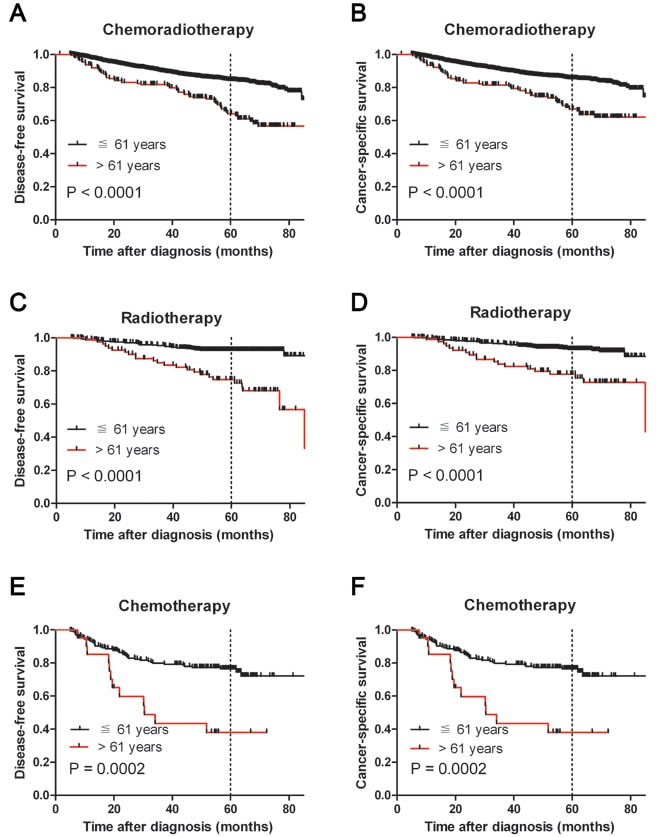
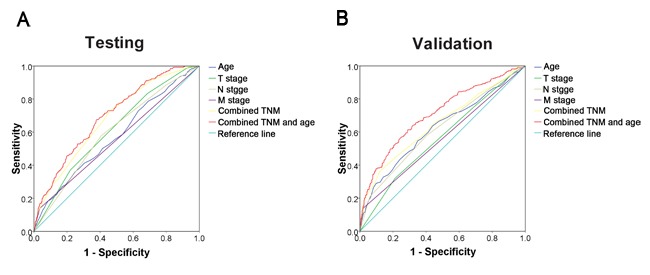
Age at diagnosis has been found to be a prognostic factor of outcomes in various cancers. However, the effect of age at diagnosis on nasopharyngeal cancer (NPC) progression has not been explored. We retrospectively evaluated the relationship between age and disease progression in 3,153 NPC patients who underwent radiotherapy, chemotherapy, or chemoradiotherapy between 2007 and 2009. Patients were randomly assigned to either a testing cohort or a validation cohort by computer-generated random assignment. X-tile plots determined the optimal cut-point of age based on survival status to be ≤61 vs. >61 years. Further correlation analysis showed that age >61 years was significantly correlated with the tumor progression and therapeutic regimen in both testing and validation cohorts (P <0.05). In the present study, we observed that older age (>61 years) was a strong and independent predictor of poor disease-free survival (DFS) and cancer-specific survival (CSS), in both univariate and multivariate analyses. Age was also found to be a significant prognostic predictor as well (P <0.05) when evaluating patients with the same disease stage. ROC analysis confirmed the predictive value of age on NPC-specific survival in both cohorts (P <0.001) and suggested that age may improve the ability to discriminate outcomes in NPCs, especially regarding tumor progression. In conclusion, our study suggests that older age at NPC diagnosis is associated with a higher incidence of tumor progression and cancer-specific mortality. Age is a strong and independent predictor of poor outcomes and may allow for more tailored therapeutic decision-making and individualized patient counseling.
Keywords: age; nasopharyngeal cancer; prognosis; tumor progression.
Conflict of interest statement
The authors have declared that no potential conflict of interest exists.
Figures
References
-
- Huang TR, Zhang SW, Chen WQ, Deng W, Zhang CY, Zhou XJ, Zhai RH. Trends in nasopharyngeal carcinoma mortality in China, 1973-2005. Asian Pacific journal of cancer prevention. 2012;13:2495–2502. - PubMed
-
- Black RJ, Bray F, Ferlay J, Parkin DM. Cancer incidence and mortality in the European Union: cancer registry data and estimates of national incidence for 1990. European journal of cancer. 1997;33:1075–1107. - PubMed
-
- Yu MC, Yuan JM. Epidemiology of nasopharyngeal carcinoma. Seminars in cancer biology. 2002;12:421–429. - PubMed
-
- Ren JS, Chen WQ, Shin HR, Ferlay J, Saika K, Zhang SW, Bray F. A comparison of two methods to estimate the cancer incidence and mortality burden in China in 2005. Asian Pacific journal of cancer prevention. 2010;11:1587–1594. - PubMed
-
- Chang ET, Adami HO. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer epidemiology, biomarkers & prevention. 2006;15:1765–1777. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
