

Efficacy and Safety of OnabotulinumtoxinA in Patients with Neurogenic Detrusor Overactivity: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 27463810
- PMCID: PMC4963110
- DOI: 10.1371/journal.pone.0159307
Efficacy and Safety of OnabotulinumtoxinA in Patients with Neurogenic Detrusor Overactivity: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
Background: Neurogenic detrusor overactivity (NDO) affects the quality of life (QoL) of millions of individuals worldwide. The purpose of this study was to assess the efficacy and safety of onabotulinumtoxinA in patients with NDO using a network meta-analytic approach, which can also quantify and compare the efficacy of onabotulinumtoxinA across different dosages.
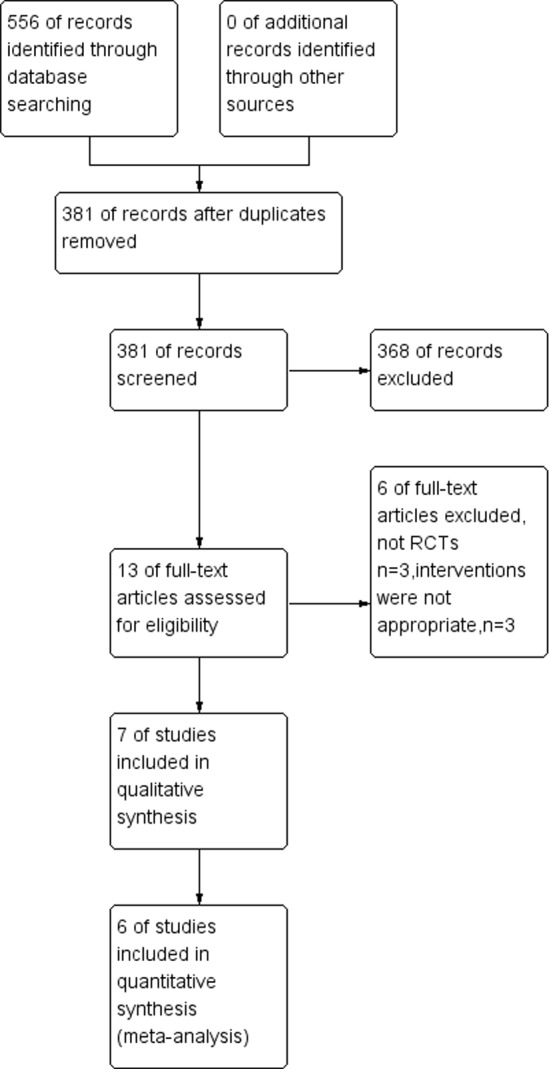
Methods: PubMed, EMBASE, and the Controlled Trials Register were searched to identify randomized controlled trials comparing onabotulinumtoxinA to a control for NDO in adult patients. The primary outcome was the mean number of urinary incontinence (UI) episodes per week. Urodynamic parameters included the maximum cystometric capacity (MCC) and the maximum detrusor pressure (MDP). The safety of onabotulinumtoxinA was determined by the incidence of various frequent adverse events (AEs). Two authors extracted data independently, and the statistical analyses were performed using RevMan 5.1.0 software.
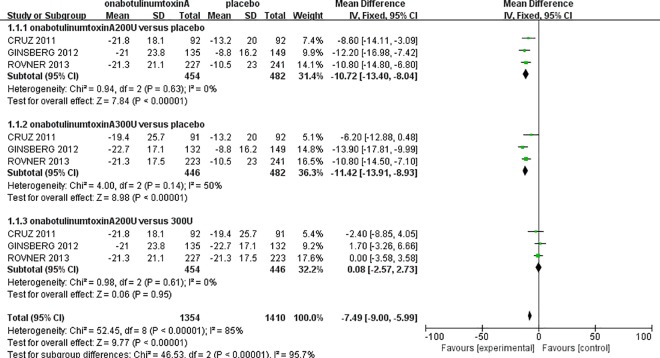
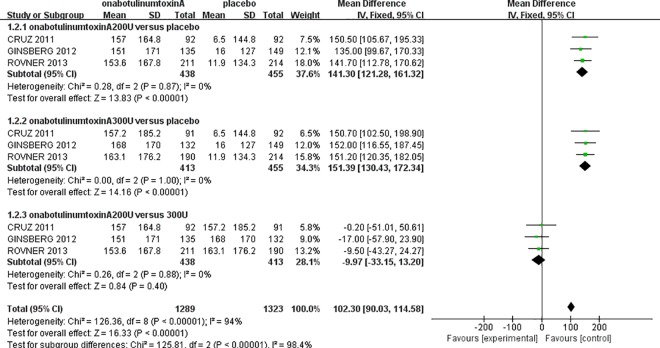
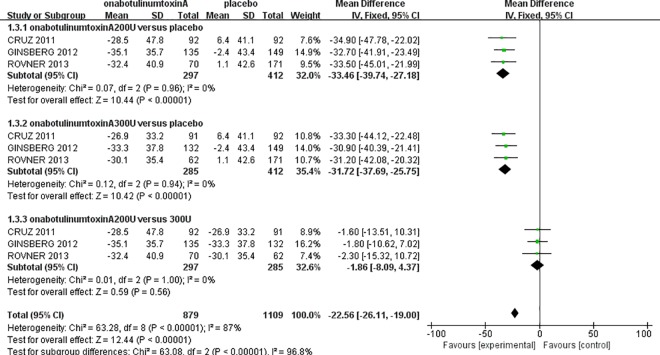
Results: A total of 1,915 patients from six randomized controlled trials were included in this meta-analysis. The onabotulinumtoxinA-treated groups had a significantly decreased mean number of urinary incontinence episodes per week (at week 6) (onabotulinumtoxinA200U: MD: -10.72, 95% CI: -13.4 to -8.04, P<0.00001; 300 U: MD: -11.42, 95% CI: -13.91 to -8.93, P<0.00001), MDP (200 U: MD: -33.46, 95% CI: -39.74 to -27.18, P<0.00001; 300 U: MD: -31.72, 95% CI: -37.69 to -25.75, P<0.00001), and greater increased MCC (200 U: MD: 141.30, 95% CI: 121.28 to 161.32, P<0.00001; 300 U: MD: 151.39, 95% CI: 130.43 to 172.34, P<0.00001) compared to the placebo-treated groups. However, there were no significant differences between the onabotulinumtoxinA-treated groups for the number of weekly UI episodes at 6 weeks (MD: 0.08, 95% CI: -2.57 to 2.73, P = 0.95). Similarly, we also observed that there were no significant differences in MCC (MD: -9.97, 95% CI: -33.15 to 13.20, P = 0.40) and MDP (MD: -1.86, 95% CI: -8.09 to 4.37, P = 0.56). Considering the AEs, the onabotulinumtoxinA-treated groups were often associated with more complications, including urinary tract infections (UTIs) (RR: 1.47, 95% CI: 1.29 to 1.67, P<0.00001), urinary retention (RR: 5.58, 95% CI: 3.53 to 8.83, P<0.00001), hematuria (RR: 1.70, 95% CI: 1.01 to 2.85, P = 0.05), and muscle weakness (RR: 2.59, 95% CI: 1.36 to 4.91, P = 0.004).
Conclusions: OnabotulinumtoxinA can significantly reduce the frequency of urge urinary incontinence and improve urodynamic parameters (MCC and MDP) in patients with NDO at 6 weeks after treatment. This meta-analysis indicates that onabotulinumtoxinA is effective and safe for treating patients with NDO compared to placebo. Additionally, we did not observe any statistical or clinical differences in efficacy between 300 and 200 U dosages.
Conflict of interest statement
Figures
Similar articles
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
An updated systematic review and statistical comparison of standardised mean outcomes for the use of botulinum toxin in the management of lower urinary tract disorders.Eur Urol. 2014 May;65(5):981-90. doi: 10.1016/j.eururo.2013.10.033. Epub 2013 Nov 1. Eur Urol. 2014. PMID: 24239446
-
Sertindole for schizophrenia.Cochrane Database Syst Rev. 2005 Jul 20;2005(3):CD001715. doi: 10.1002/14651858.CD001715.pub2. Cochrane Database Syst Rev. 2005. PMID: 16034864 Free PMC article.
-
Botulinum toxin type A therapy for cervical dystonia.Cochrane Database Syst Rev. 2017 Dec 12;12(12):CD003633. doi: 10.1002/14651858.CD003633.pub3. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Nov 12;11:CD003633. doi: 10.1002/14651858.CD003633.pub4. PMID: 29230798 Free PMC article. Updated.
Cited by
-
A systematic review and meta-analysis of effectiveness and safety of therapy for overactive bladder using botulinum toxin A at different dosages.Oncotarget. 2017 Aug 7;8(52):90338-90350. doi: 10.18632/oncotarget.20056. eCollection 2017 Oct 27. Oncotarget. 2017. PMID: 29163833 Free PMC article.
-
Long-term follow-up of intradetrusor botulinum toxin utilisation: A comparison of patients with multiple sclerosis and idiopathic overactive bladder.BJUI Compass. 2024 Dec 19;6(1):e479. doi: 10.1002/bco2.479. eCollection 2025 Jan. BJUI Compass. 2024. PMID: 39877585 Free PMC article.
-
Botulinum Toxin A: A Review of Potential Uses in Treatment of Female Urogenital and Pelvic Floor Disorders.Ochsner J. 2020 Winter;20(4):400-409. doi: 10.31486/toj.19.0076. Ochsner J. 2020. PMID: 33408578 Free PMC article. Review.
-
Neuromyelitis optica in a young patient presenting with urinary retention: A case report.Urol Case Rep. 2023 Jun 5;50:102460. doi: 10.1016/j.eucr.2023.102460. eCollection 2023 Sep. Urol Case Rep. 2023. PMID: 37358990 Free PMC article.
-
Stem Cell Therapy in Spinal Cord Injury-Induced Neurogenic Lower Urinary Tract Dysfunction.Stem Cell Rev Rep. 2023 Aug;19(6):1691-1708. doi: 10.1007/s12015-023-10547-9. Epub 2023 Apr 28. Stem Cell Rev Rep. 2023. PMID: 37115409 Review.
References
-
- Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21: 167–178. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
