

Disruption of desmin-mitochondrial architecture in patients with regurgitant mitral valves and preserved ventricular function
- PMID: 27464577
- PMCID: PMC5199142
- DOI: 10.1016/j.jtcvs.2016.06.017
Disruption of desmin-mitochondrial architecture in patients with regurgitant mitral valves and preserved ventricular function
Abstract
Objective: Recent studies have demonstrated improved outcomes in patients receiving early surgery for degenerative mitral regurgitation (MR) rather than adhering to conventional guidelines for surgical intervention. However, studies providing a mechanistic basis for these findings are limited.
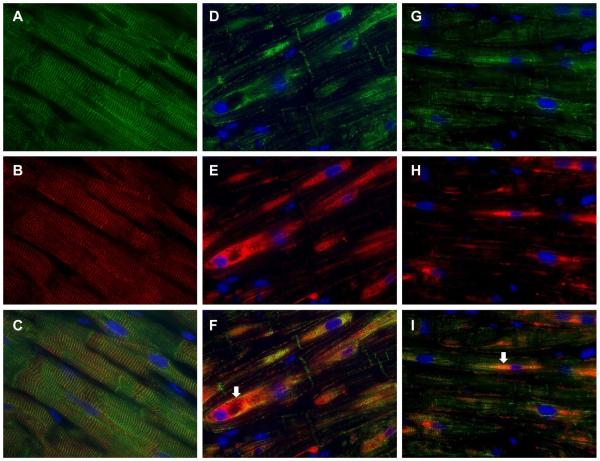
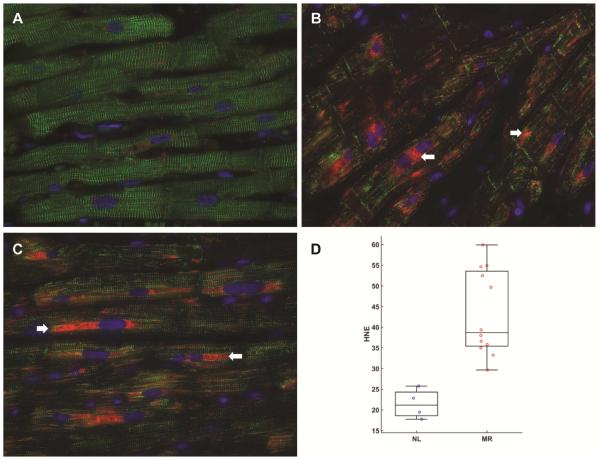
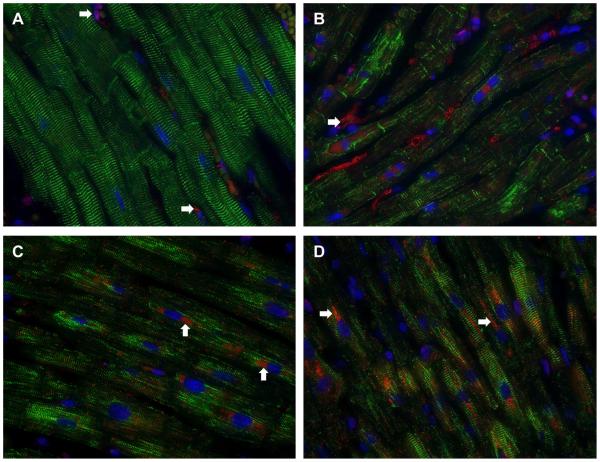
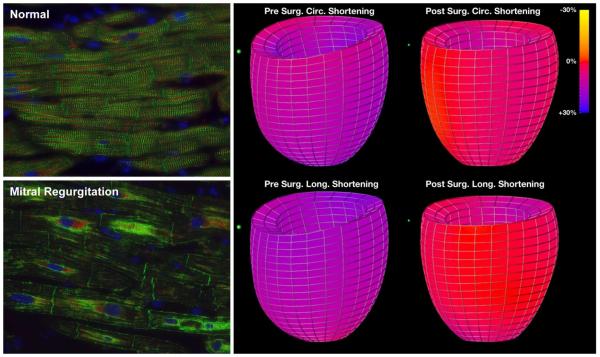
Methods: Left ventricular (LV) myocardium from 22 patients undergoing mitral valve repair for American Heart Association class I indications was evaluated for desmin, the voltage-dependent anion channel, α-B-crystallin, and α, β-unsaturated aldehyde 4-hydroxynonenal by fluorescence microscopy. The same was evaluated in 6 normal control LV autopsy specimens. Cardiomyocyte ultrastructure was examined by transmission electron microscopy. Magnetic resonance imaging with tissue tagging was performed in 55 normal subjects and 22 MR patients before and 6 months after mitral valve repair.
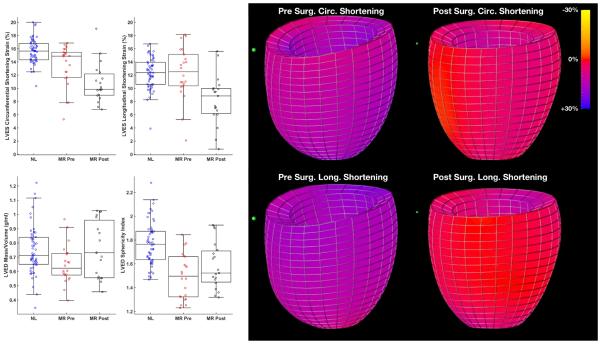
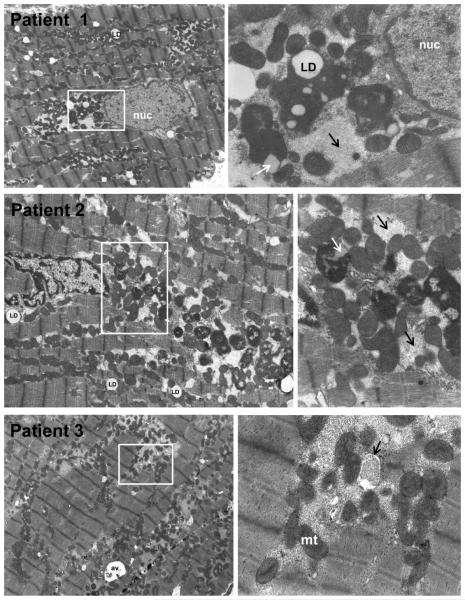
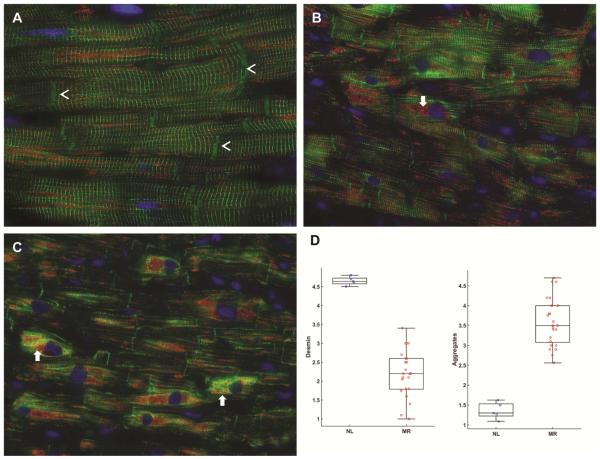
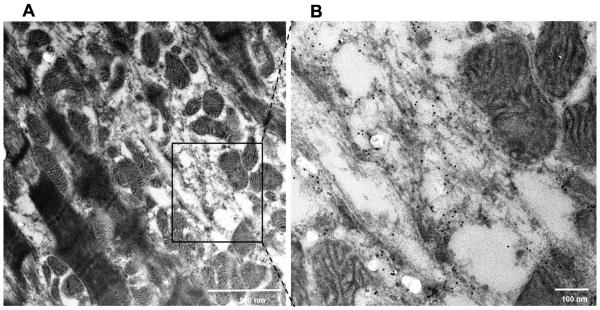
Results: LV end-diastolic volume was 1.5-fold (P < .0001) higher and LV mass-to-volume ratio was lower in MR (P = .004) hearts versus normal hearts and showed improvement 6 months after mitral valve surgery. However, LV ejection fraction decreased from 65% ± 7% to 52% ± 9% (P < .0001) and LV circumferential (P < .0001) and longitudinal strain decreased significantly below normal values (P = .002) after surgery. Hearts with MR had a 53% decrease in desmin (P < .0001) and a 2.6-fold increase in desmin aggregates (P < .0001) versus normal, along with substantial, intense perinuclear staining of α, β-unsaturated aldehyde 4-hydroxynonenal in areas of mitochondrial breakdown and clustering. Transmission electron microscopy demonstrated numerous electron-dense deposits, myofibrillar loss, Z-disc abnormalities, and extensive granulofilamentous debris identified as desmin-positive by immunogold transmission electron microscopy.
Conclusions: Despite well-preserved preoperative LV ejection fraction, severe oxidative stress and disruption of cardiomyocyte desmin-mitochondrial sarcomeric architecture may explain postoperative LV functional decline and further supports the move toward earlier surgical intervention.
Keywords: cardiomyocyte; heart failure; mitochondria; mitral regurgitation.
Published by Elsevier Inc.
Figures
Comment in
-
Left ventricular dysfunction after degenerative mitral valve repair: A question of better molecular targets or better surgical timing?J Thorac Cardiovasc Surg. 2016 Oct;152(4):1071-4. doi: 10.1016/j.jtcvs.2016.07.018. Epub 2016 Jul 27. J Thorac Cardiovasc Surg. 2016. PMID: 27523402 No abstract available.
References
-
- Enriquez-Sarano M, Akins CW, Vahanian A. Mitral regurgitation. Lancet. 2009;373:1382–94. - PubMed
-
- Suri RM, Aviernos J-F, Dearani JA, Mahoney DW, Michelena HI, Schaff HV, Enriquez-Sarano M. Management of less-than-severe mitral regurgitation: should guidelines recommend earlier surgical intervention. Eur J Cardiovasc Surg. 2011;40:496–502. - PubMed
-
- Enriquez-Sarano M, Avierinos JF, Messika-Zeitoun D, Detaint D, Capps M, Nkomo V, et al. Quantitative determinants of the outcome of asymptomatic mitral regurgitation. N Eng J Med. 2005;352:875–83. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, III, Guyton RA, et al. 2014 AHA/ACC Guideline for the management of patients with valvular heart disease: report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:2440–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
