

The use of mosquito repellents at three sites in India with declining malaria transmission: surveys in the community and clinic
- PMID: 27465199
- PMCID: PMC4963934
- DOI: 10.1186/s13071-016-1709-9
The use of mosquito repellents at three sites in India with declining malaria transmission: surveys in the community and clinic
Abstract
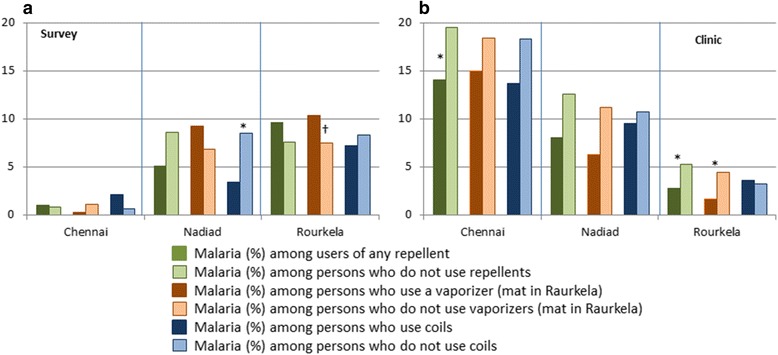
Background: Repellents such as coils, vaporizers, mats and creams can be used to reduce the risk of malaria and other infectious diseases. Although evidence for their effectiveness is limited, they are advertised as providing an additional approach to mosquito control in combination with other strategies, e.g. insecticide-treated nets. We examined the use of repellents in India in an urban setting in Chennai (mainly Plasmodium vivax malaria), a peri-urban setting in Nadiad (both P. vivax and P. falciparum malaria), and a more rural setting in Raurkela (mainly P. falciparum malaria).
Methods: The use of repellents was examined at the household level during a census, and at the individual level in cross-sectional surveys and among patients visiting a clinic with fever or other symptoms. Factors associated with their use were examined in a multivariate analysis, and the association between malaria and the use of repellents was assessed among survey- and clinic participants.
Results: Characteristics of participants differed by region, with more people of higher education present in Chennai. Use of repellents varied between 56-77 % at the household level and between 32-78 % at the individual level. Vaporizers were the main repellents used in Chennai, whereas coils were more common in Nadiad and Raurkela. In Chennai and Nadiad, vaporizers were more likely to be used in households with young male children. Vaporizer use was associated with higher socio-economic status (SES) in households in Chennai and Nadiad, whereas use of coils was greater in the lower SES strata. In Raurkela, there was a higher use of coils among the higher SES strata. Education was associated with the use of a repellent among survey participants in Chennai and clinic study participants in Chennai and Nadiad. Repellent use was associated with less malaria in the clinic study in Chennai and Raurkela, but not in the surveys, with the exception of the use of coils in Nadiad.
Conclusions: Repellents are widely used in India. Their use is influenced by the level of education and SES. Information on effectiveness and guidance on choices may improve rational use.
Keywords: Education; Mosquito control; Plasmodium falciparum; Plasmodium vivax; Repellents; Rural; Socio-economic status; Urban.
Figures


References
-
- Global Malaria Programme WHO. World Malaria Report 2015. Geneva: World Health Organization; 2015.
-
- National Vector Borne Disease Control Programme, Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India. Annual Report 2011–12. New Delhi, India: Government of India 2012. http://www.nvbdcp.gov.in/Doc/Annual-report-2011-12-NVBDCP.pdf. Accessed 13 07 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
