

Uterine fibroid management: from the present to the future
- PMID: 27466209
- PMCID: PMC5853598
- DOI: 10.1093/humupd/dmw023
Uterine fibroid management: from the present to the future
Abstract
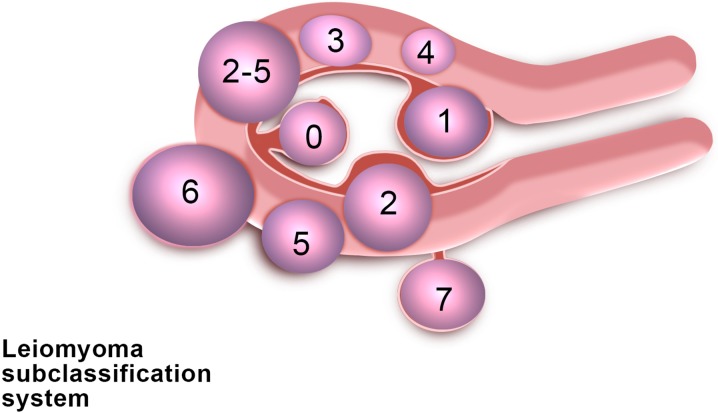
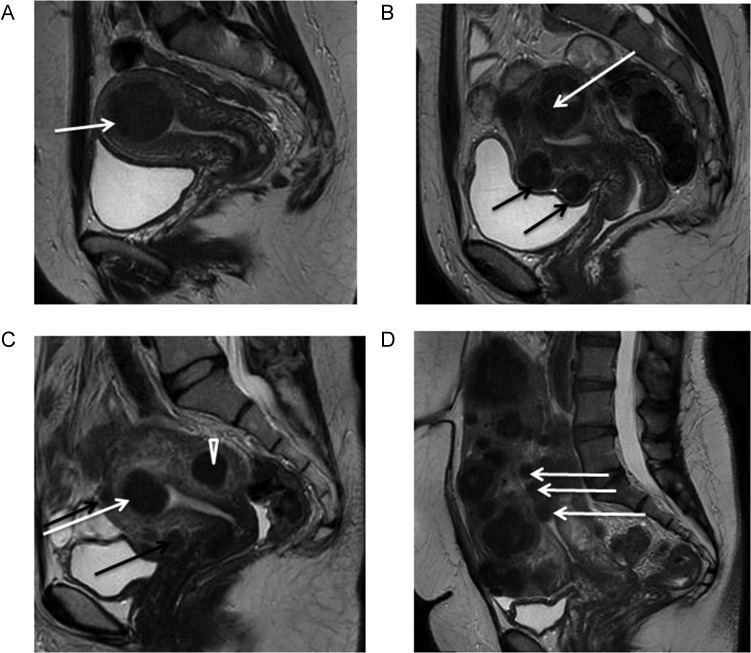
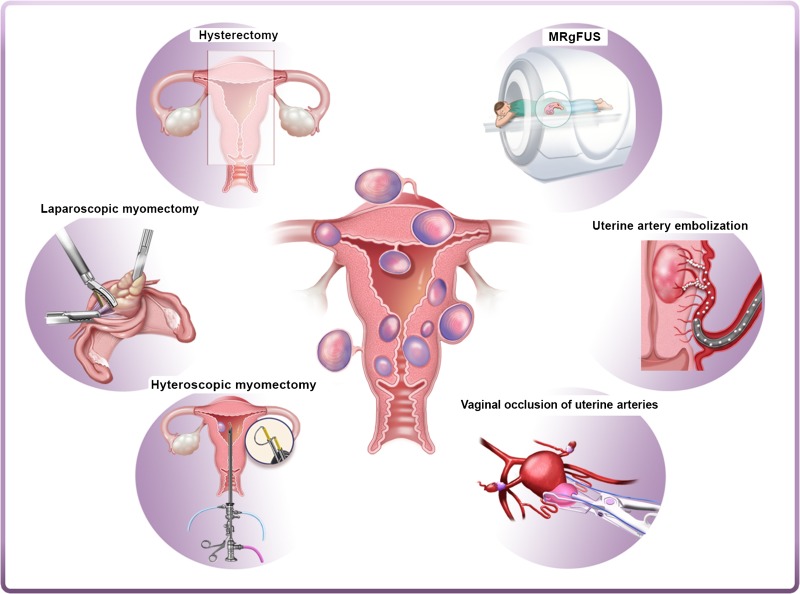
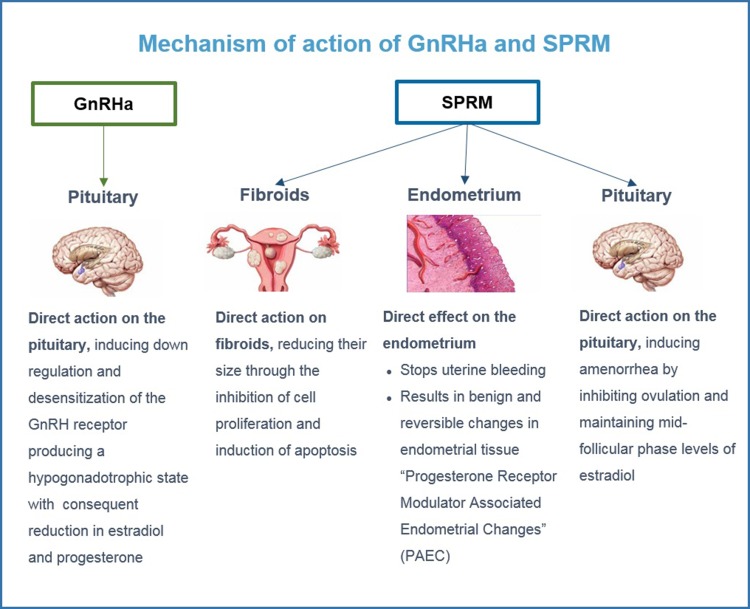
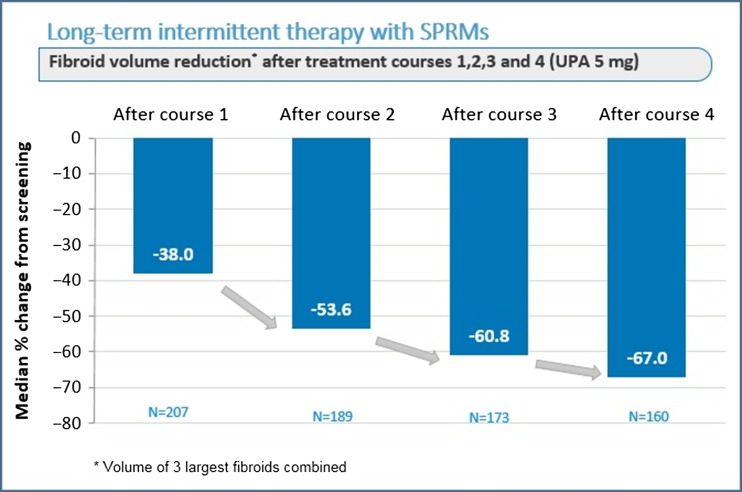
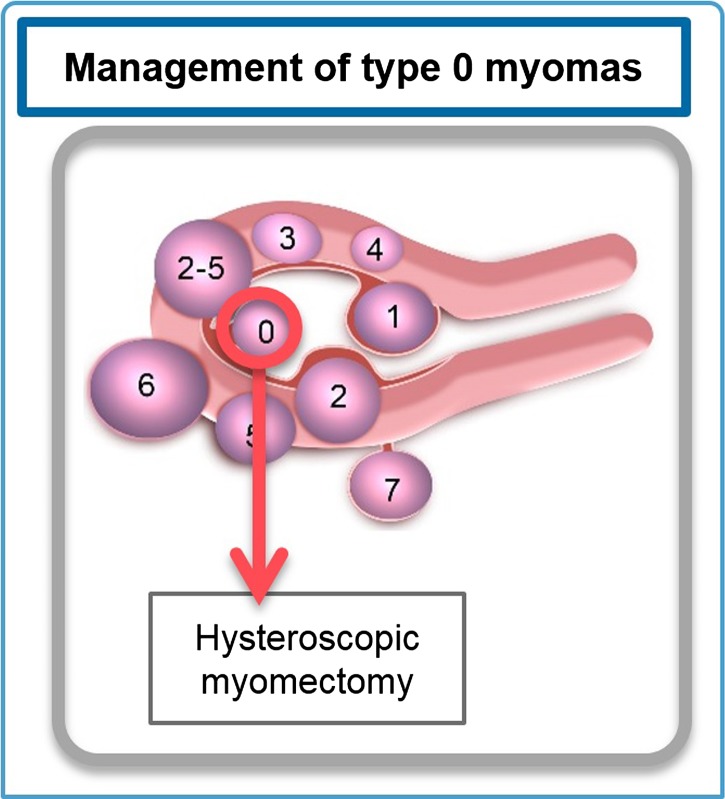
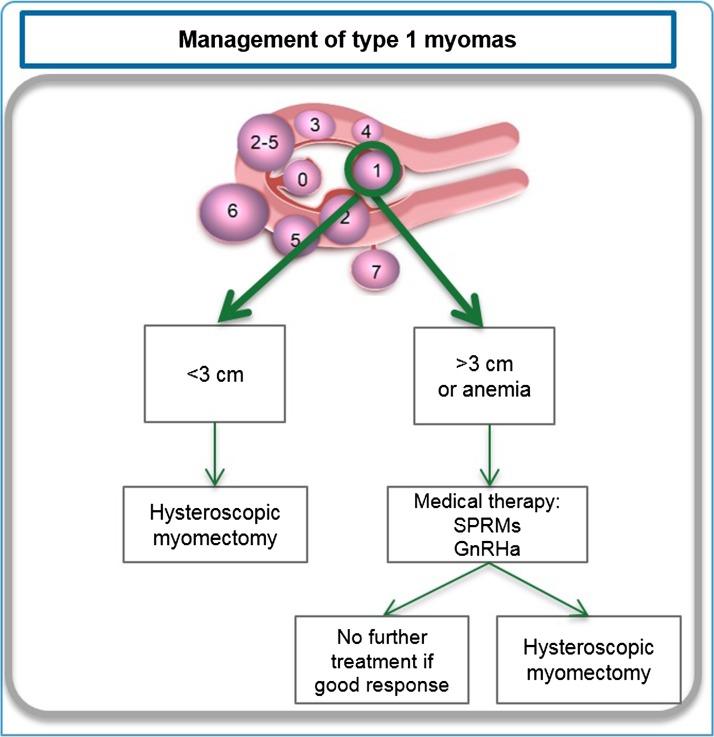
Uterine fibroids (also known as leiomyomas or myomas) are the most common form of benign uterine tumors. Clinical presentations include abnormal bleeding, pelvic masses, pelvic pain, infertility, bulk symptoms and obstetric complications.Almost a third of women with leiomyomas will request treatment due to symptoms. Current management strategies mainly involve surgical interventions, but the choice of treatment is guided by patient's age and desire to preserve fertility or avoid 'radical' surgery such as hysterectomy. The management of uterine fibroids also depends on the number, size and location of the fibroids. Other surgical and non-surgical approaches include myomectomy by hysteroscopy, myomectomy by laparotomy or laparoscopy, uterine artery embolization and interventions performed under radiologic or ultrasound guidance to induce thermal ablation of the uterine fibroids.There are only a few randomized trials comparing various therapies for fibroids. Further investigations are required as there is a lack of concrete evidence of effectiveness and areas of uncertainty surrounding correct management according to symptoms. The economic impact of uterine fibroid management is significant and it is imperative that new treatments be developed to provide alternatives to surgical intervention.There is growing evidence of the crucial role of progesterone pathways in the pathophysiology of uterine fibroids due to the use of selective progesterone receptor modulators (SPRMs) such as ulipristal acetate (UPA). The efficacy of long-term intermittent use of UPA was recently demonstrated by randomized controlled studies.The need for alternatives to surgical intervention is very real, especially for women seeking to preserve their fertility. These options now exist, with SPRMs which are proven to treat fibroid symptoms effectively. Gynecologists now have new tools in their armamentarium, opening up novel strategies for the management of uterine fibroids.
Keywords: leiomyomas; medical therapy; myomectomy; selective progesterone receptor modulators; surgery; ulipristal acetate; uterine fibroids.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Alborzi S, Ghannadan E, Alborzi S, Alborzi M.. A comparison of combined laparoscopic uterine artery ligation and myomectomy versus laparoscopic myomectomy in treatment of symptomatic myoma. Fertil Steril 2009;92:742–747. - PubMed
-
- Alessandri F, Lijoi D, Mistrangelo E, Ferrero S, Ragni N.. Randomized study of laparoscopic versus minilaparotomic myomectomy for uterine myomas. J Minim Invasive Gynecol 2006;13:92–97. - PubMed
-
- American College of Obstetricians and Gynecologists ACOG practice bulletin: alternatives to hysterectomy in the management of leiomyomas. Obstet Gynecol 2008;112:387–400. - PubMed
-
- Andreotti RF, Fleischer AC.. Practical applications of 3D sonography in gynecologic imaging. Radiol Clin North Am. 2014;52:1201–1213. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
