

Misinterpretation of ischaemic infarct location in relationship to the cerebrovascular territories
- PMID: 27466359
- PMCID: PMC5036207
- DOI: 10.1136/jnnp-2015-312906
Misinterpretation of ischaemic infarct location in relationship to the cerebrovascular territories
Abstract
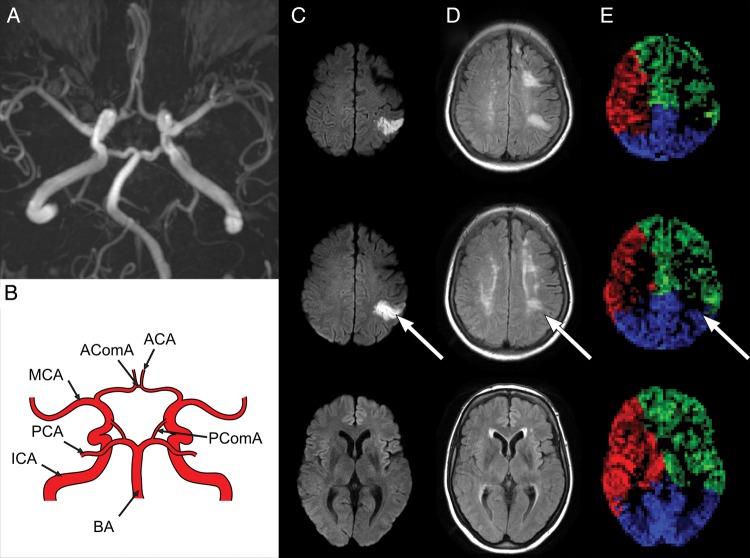
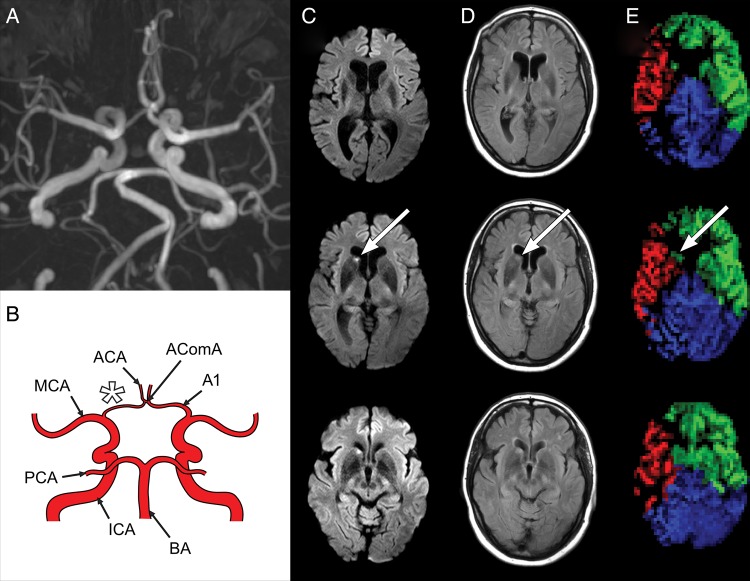
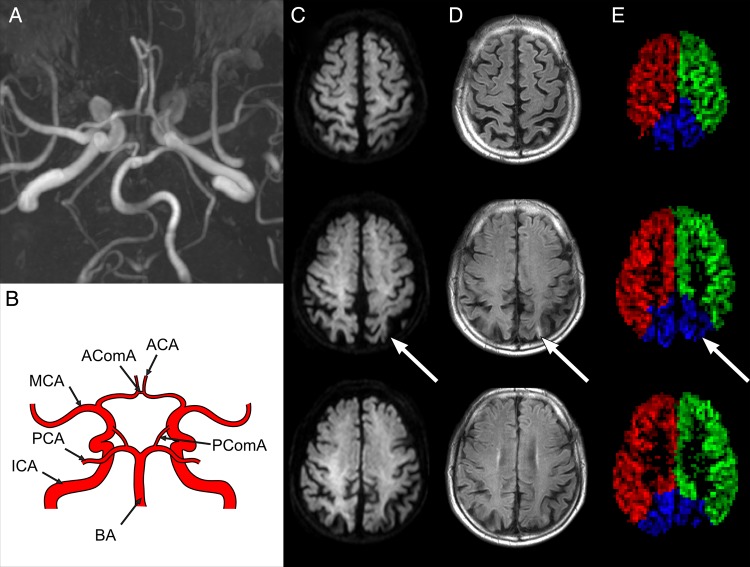
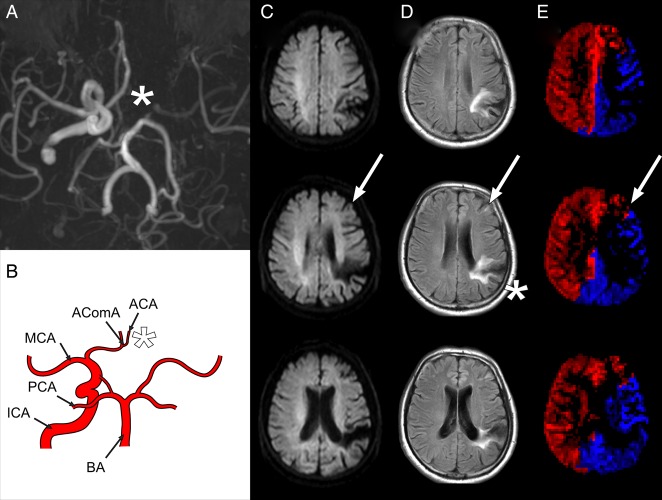
Purpose: Cerebral perfusion territories are known to vary widely among individuals. This may lead to misinterpretation of the symptomatic artery in patients with ischaemic stroke to a wrong assumption of the underlying aetiology being thromboembolic or hypoperfusion. The aim of the present study was to investigate such potential misinterpretation with territorial arterial spin labelling (T-ASL) by correlating infarct location with imaging of the perfusion territory of the carotid arteries or basilar artery.
Materials and methods: 223 patients with subacute stroke underwent MRI including structural imaging scans to determine infarct location, time-of-flight MR angiography (MRA) to determine the morphology of the circle of Willis and T-ASL to identify the perfusion territories of the internal carotid arteries, and basilar artery. Infarct location and the perfusion territory of its feeding artery were classified with standard MRI and MRA according to a perfusion atlas, and were compared to the classification made according to T-ASL.
Results: A total of 149 infarctions were detected in 87 of 223 patients. 15 out of 149 (10%) infarcts were erroneously attributed to a single perfusion territory; these infarcts were partly located in the originally determined perfusion territory but proved to be localised in the border zone with the adjacent perfusion territory instead. 12 out of 149 (8%) infarcts were misclassified with standard assessments and were not located in the original perfusion territory.
Conclusions: T-ASL with territorial perfusion imaging may provide important additional information for classifying the symptomatic brain-feeding artery when compared to expert evaluation with MRI and MRA.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical