

HIV DNA Is Frequently Present within Pathologic Tissues Evaluated at Autopsy from Combined Antiretroviral Therapy-Treated Patients with Undetectable Viral Loads
- PMID: 27466426
- PMCID: PMC5044815
- DOI: 10.1128/JVI.00674-16
HIV DNA Is Frequently Present within Pathologic Tissues Evaluated at Autopsy from Combined Antiretroviral Therapy-Treated Patients with Undetectable Viral Loads
Abstract
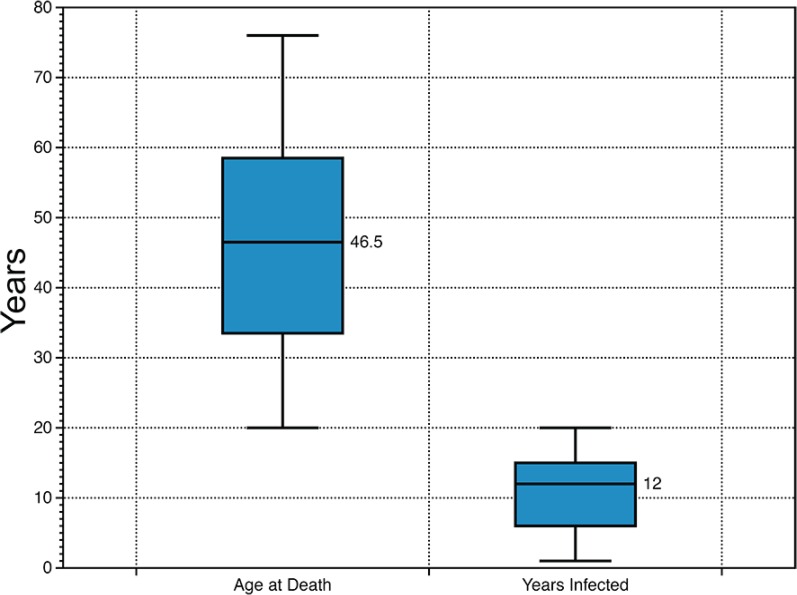
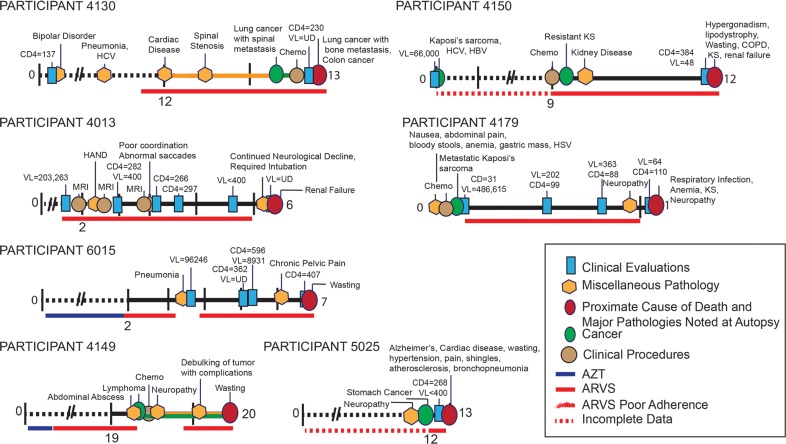
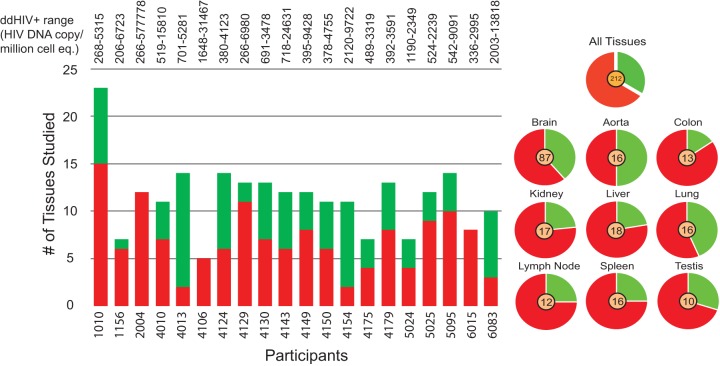
HIV infection treatment strategies have historically defined effectiveness through measuring patient plasma HIV RNA. While combined antiretroviral therapy (cART) can reduce plasma viral load (pVL) to undetectable levels, the degree that HIV is eliminated from other anatomical sites remains unclear. We investigated the HIV DNA levels in 229 varied autopsy tissues from 20 HIV-positive (HIV(+)) cART-treated study participants with low or undetectable plasma VL and cerebrospinal fluid (CSF) VL prior to death who were enrolled in the National Neurological AIDS Bank (NNAB) longitudinal study and autopsy cohort. Extensive medical histories were obtained for each participant. Autopsy specimens, including at least six brain and nonbrain tissues per participant, were reviewed by study pathologists. HIV DNA, measured in tissues by quantitative and droplet digital PCR, was identified in 48/87 brain tissues and 82/142 nonbrain tissues at levels >200 HIV copies/million cell equivalents. No participant was found to be completely free of tissue HIV. Parallel sequencing studies from some tissues recovered intact HIV DNA and RNA. Abnormal histological findings were identified in all participants, especially in brain, spleen, lung, lymph node, liver, aorta, and kidney. All brain tissues demonstrated some degree of pathology. Ninety-five percent of participants had some degree of atherosclerosis, and 75% of participants died with cancer. This study assists in characterizing the anatomical locations of HIV, in particular, macrophage-rich tissues, such as the central nervous system (CNS) and testis. Additional studies are needed to determine if the HIV recovered from tissues promotes the pathogenesis of inflammatory diseases, such as HIV-associated neurocognitive disorders, cancer, and atherosclerosis.
Importance: It is well-known that combined antiretroviral therapy (cART) can reduce plasma HIV to undetectable levels; however, cART cannot completely clear HIV infection. An ongoing question is, "Where is HIV hiding?" A well-studied HIV reservoir is "resting" T cells, which can be isolated from blood products and succumb to cART once activated. Less-studied reservoirs are anatomical tissue samples, which have unknown cART penetration, contain a comparably diverse spectrum of potentially HIV-infected immune cells, and are important since <2% of body lymphocytes actually reside in blood. We examined 229 varied autopsy specimens from 20 HIV(+) participants who died while on cART and identified that >50% of tissues were HIV infected. Additionally, we identified considerable pathology in participants' tissues, especially in brain, spleen, lung, lymph node, liver, aorta, and kidney. This study substantiates that tissue-associated HIV is present despite cART and can inform future studies into HIV persistence.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Kurz M, Burkhalter F, Dickenmann M, Hopfer H, Mayr M, Elzi L, Battegay M. 2015. Acute kidney injury KDIGO stage 2 to 3 in HIV-positive patients treated with cART–a case series over 11 years in a cohort of 1,153 patients. Swiss Med Wkly 145:w14135. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
