

Long-term outcomes after multidisciplinary management of T3 laryngeal squamous cell carcinomas: Improved functional outcomes and survival with modern therapeutic approaches
- PMID: 27466789
- PMCID: PMC5539952
- DOI: 10.1002/hed.24532
Long-term outcomes after multidisciplinary management of T3 laryngeal squamous cell carcinomas: Improved functional outcomes and survival with modern therapeutic approaches
Erratum in
-
Erratum.Head Neck. 2017 Jul;39(7):1484-1496. doi: 10.1002/hed.24753. Epub 2017 Apr 7. Head Neck. 2017. PMID: 28608443 No abstract available.
Abstract
Background: The purpose of this study was to evaluate the long-term outcomes after initial definitive or adjuvant radiotherapy (RT) for T3 laryngeal cancers.
Methods: We reviewed 412 patients treated for T3 laryngeal squamous cell cancer from 1985 to 2011.
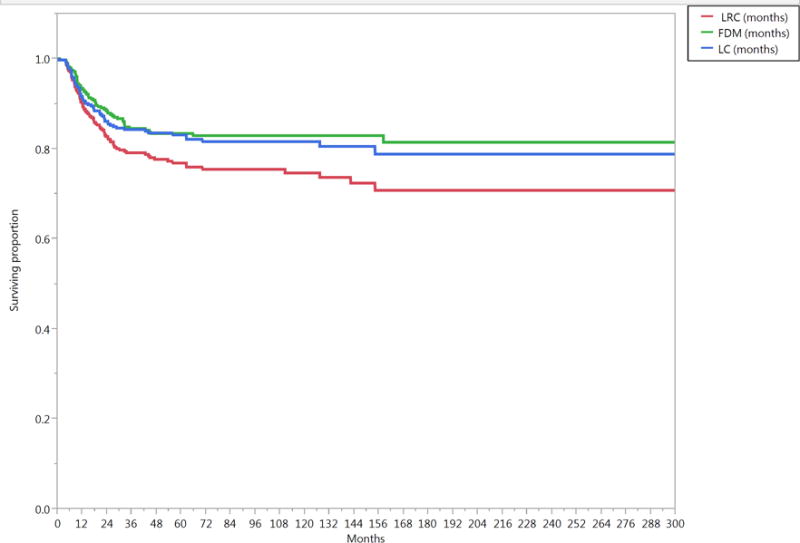
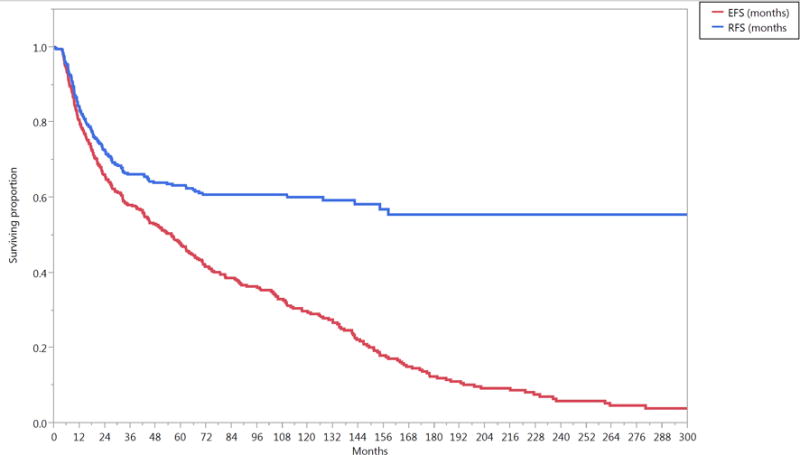
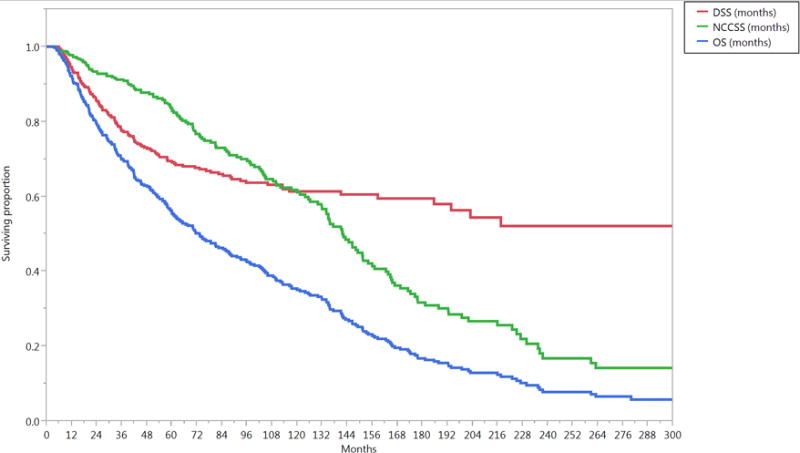
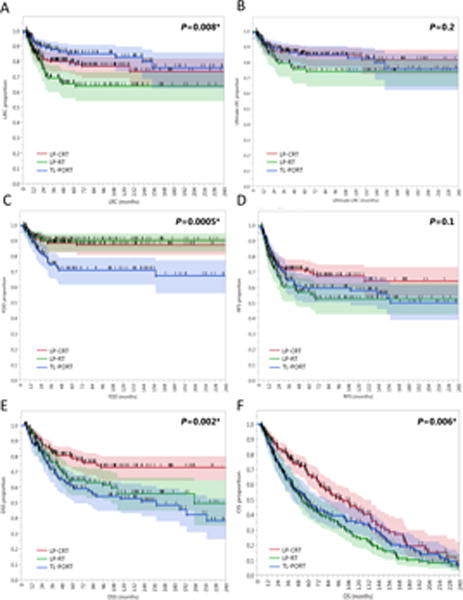
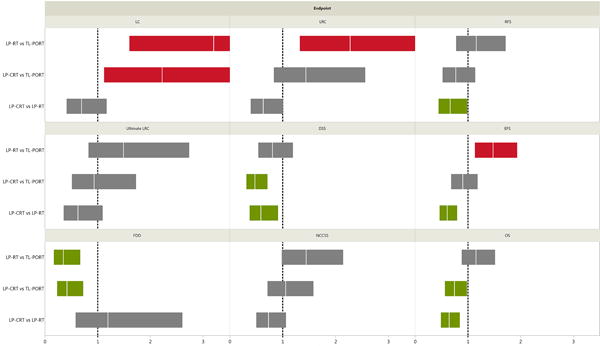
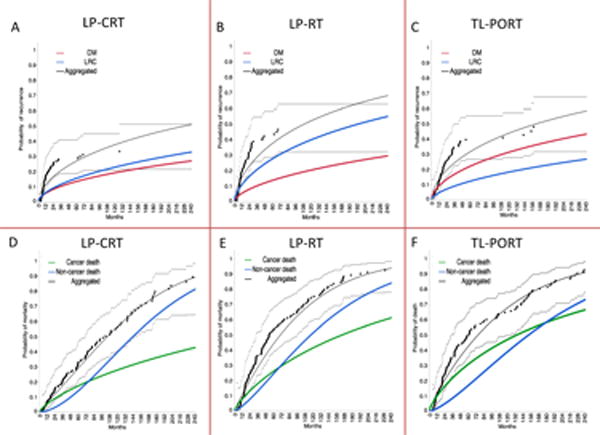
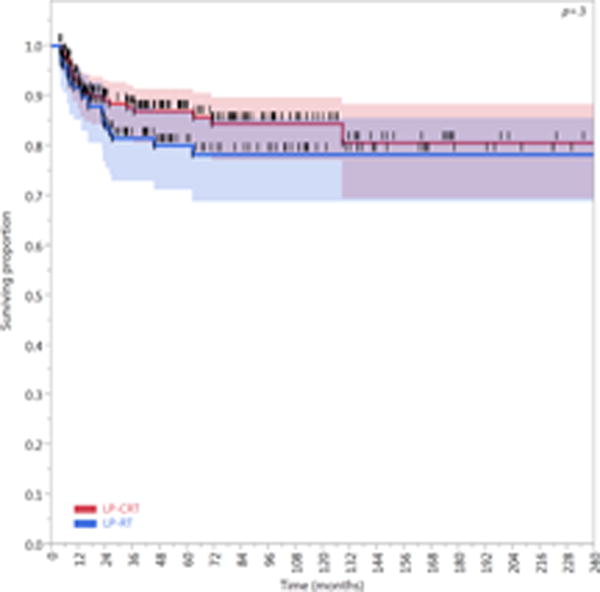
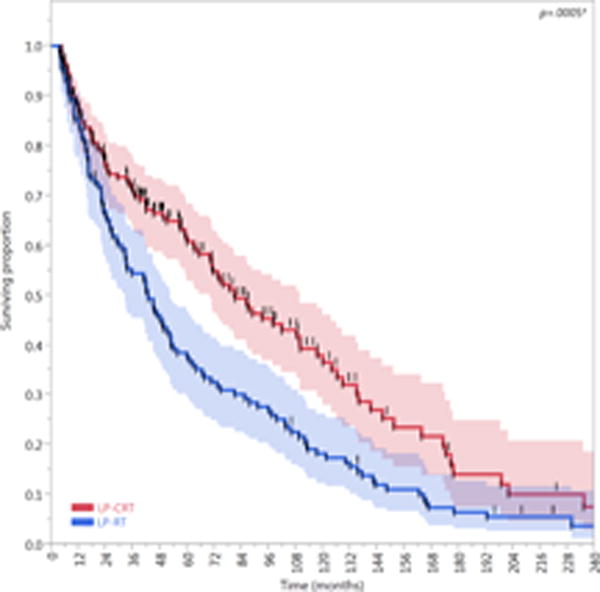
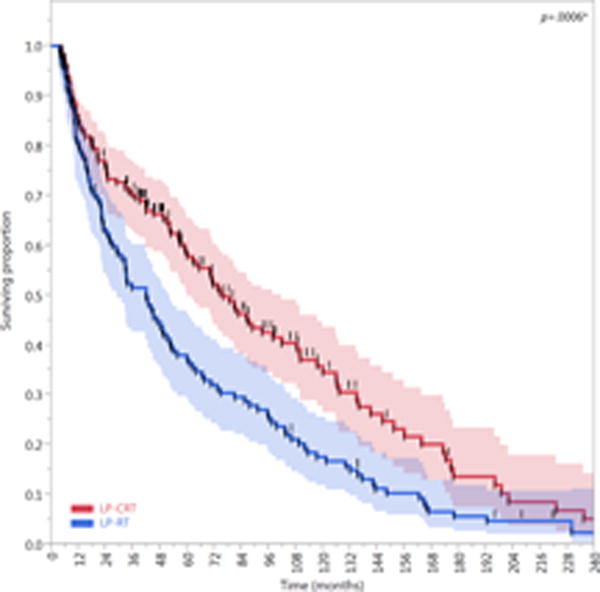
Results: The 10-year overall survival (OS) was 35%; disease-specific-survival (DSS) was 61%; locoregional control was 76%; and freedom from distant metastasis was 83%. Chemotherapy, age, performance status <2, node-negative status, and glottic subsite were associated with improved survival (all p < .03). Larynx preservation with induction and/or concurrent chemoradiotherapy (LP-CRT) had better laryngectomy-free survival than RT alone (LP-RT; hazard ratio [HR] = 0.62; 95% confidence interval [CI] = 0.47-0.81; p = .0005); 10-year laryngectomy-free survival rates of the LP-CRT cohort (37%) were higher than those of the LP-RT cohort (18%). The 5-year DSS and OS rates of the LP-CRT cohort (79% and 67%) were better after total laryngectomy with postoperative RT (TL-PORT; 61% and 50%) and LP-RT (64% and 46%; p < .006 for all).
Conclusion: In patients with T3 laryngeal cancers, LP-CRT provides better functional, oncologic, and survival outcomes than historical TL-PORT or LP-RT does. © 2016 Wiley Periodicals, Inc. Head Neck 38: 1739-1751, 2016.
Keywords: T3; outcomes; radiotherapy; survival; total laryngectomy.
© 2016 Wiley Periodicals, Inc.
Figures

References
-
- Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. The Department of Veterans Affairs Laryngeal Cancer Study Group. N Engl J Med. 1991;324(24):1685–90. - PubMed
-
- Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003;349(22):2091–8. - PubMed
-
- Hoffman HT, Porter K, Karnell LH, et al. Laryngeal cancer in the United States: changes in demographics, patterns of care, and survival. Laryngoscope. 2006;116(9 Pt 2 Suppl 111):1–13. - PubMed
-
- Gourin CG, Conger BT, Sheils WC, Bilodeau PA, Coleman TA, Porubsky ES. The effect of treatment on survival in patients with advanced laryngeal carcinoma. Laryngoscope. 2009;119(7):1312–7. - PubMed
-
- Dziegielewski PT, O’Connell DA, Klein M, et al. Primary total laryngectomy versus organ preservation for T3/T4a laryngeal cancer: a population-based analysis of survival. J Otolaryngol Head Neck Surg. 2012;41(Suppl 1):S56–64. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
