

Ultrasound as an Adjunct to Mammography for Breast Cancer Screening: A Health Technology Assessment
- PMID: 27468326
- PMCID: PMC4947971
Ultrasound as an Adjunct to Mammography for Breast Cancer Screening: A Health Technology Assessment
Abstract
Background: Screening with mammography can detect breast cancer early, before clinical symptoms appear. Some cancers, however, are not captured with mammography screening alone. Ultrasound has been suggested as a safe adjunct screening tool that can detect breast cancers missed on mammography. We investigated the benefits, harms, cost-effectiveness, and cost burden of ultrasound as an adjunct to mammography compared with mammography alone for screening women at average risk and at high risk for breast cancer.
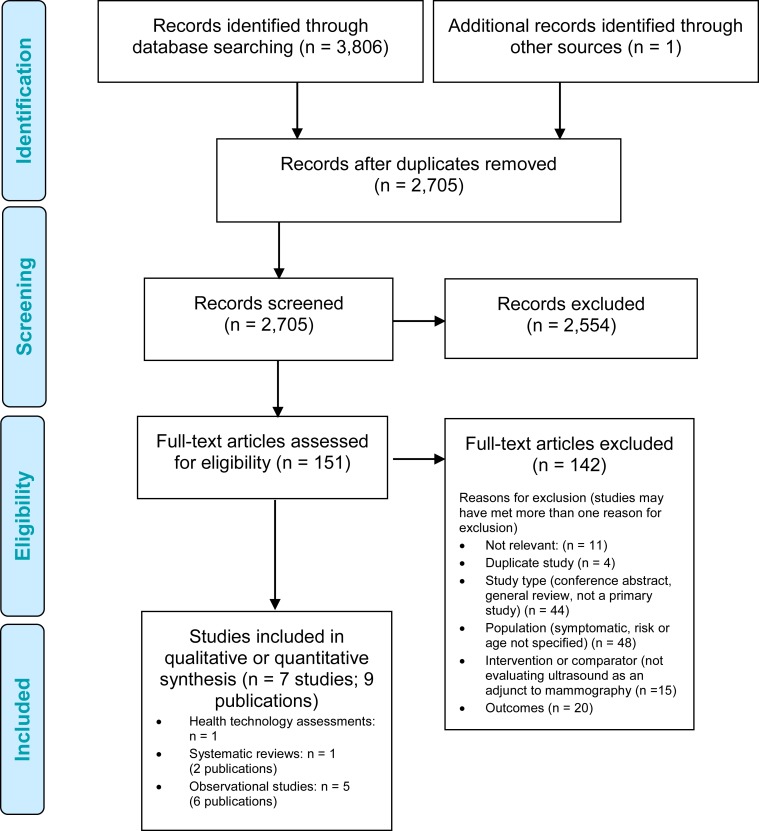
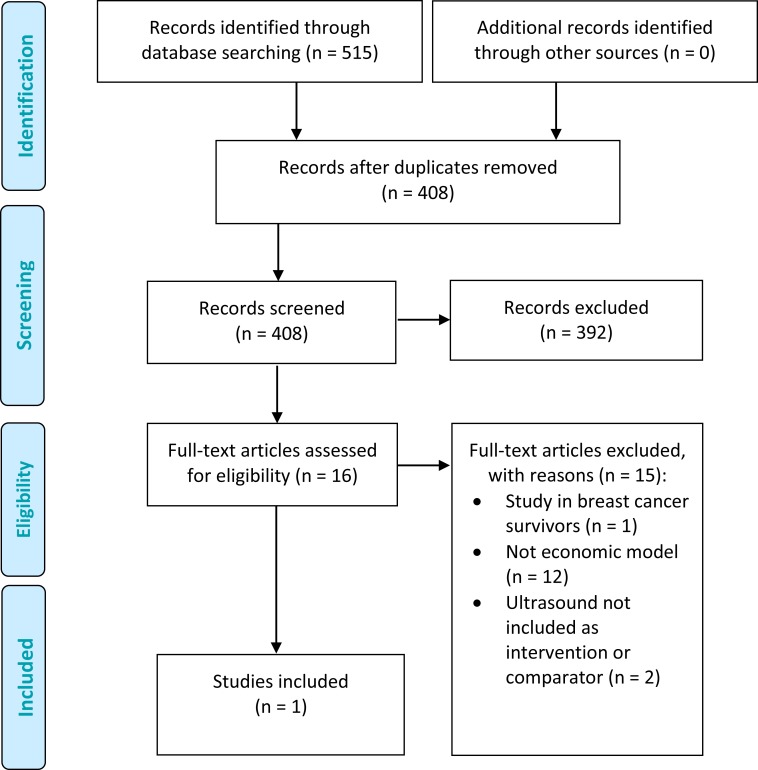
Methods: We searched Ovid MEDLINE, Ovid Embase, EBM Reviews, and the NHS Economic Evaluation Database, from January 1998 to June 2015, for evidence of effectiveness, harms, diagnostic accuracy, and cost-effectiveness. Only studies evaluating the use of ultrasound as an adjunct to mammography in the specified populations were included. We also conducted a cost analysis to estimate the costs in Ontario over the next 5 years to fund ultrasound as an adjunct to mammography in breast cancer screening for high-risk women who are contraindicated for MRI, the current standard of care to supplement mammography.
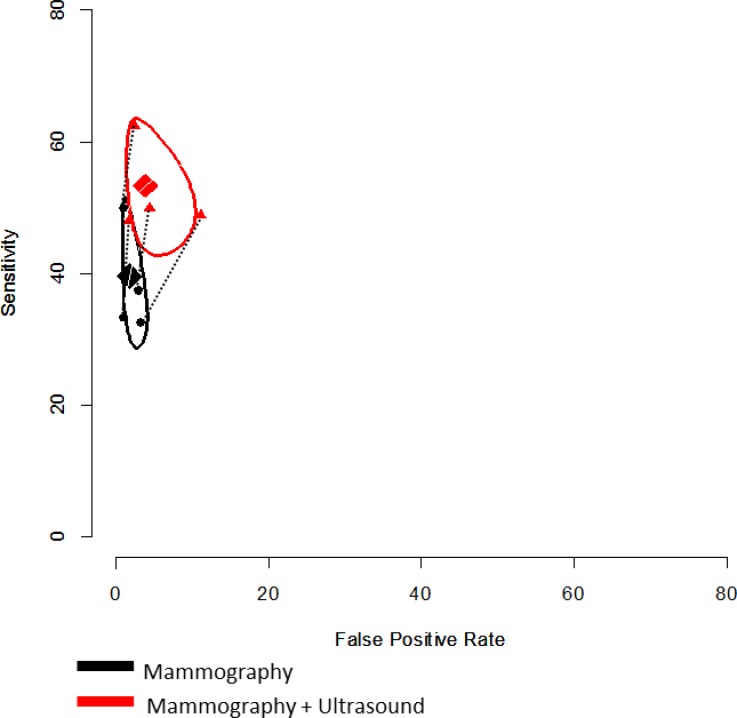
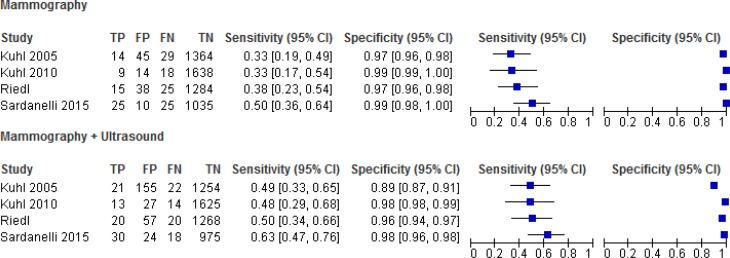
Results: No studies in average-risk women met the inclusion criteria of the clinical review. We included 5 prospective, paired cohort studies in high-risk women, 4 of which were relevant to the Ontario context. Adjunct ultrasound identified between 2.3 and 5.9 additional breast cancers per 1,000 screens. The average pooled sensitivity of mammography and ultrasound was 53%, a statistically significant increase relative to mammography alone (absolute increase 13%; P < .05). The average pooled specificity of the combined test was 96%, an absolute increase in the false-positive rate of 2% relative to mammography screening alone. The GRADE for this body of evidence was low. Additional annual costs of using breast ultrasound as an adjunct to mammography for high-risk women in Ontario contraindicated for MRI would range from $15,500 to $30,250 in the next 5 years.
Conclusions: We found no evidence that evaluated the comparative effectiveness or diagnostic accuracy of screening breast ultrasound as an adjunct to mammography among average-risk women aged 50 years and over. In women at high risk of developing breast cancer, there is low-quality evidence that screening with mammography and adjunct ultrasound detects additional cases of disease, with improved sensitivity compared to mammography alone. Screening with adjunct ultrasound also increases the number of false-positive findings and subsequent biopsy recommendations. It is unclear if the use of screening breast ultrasound as an adjunct to mammography will reduce breast cancer-related mortality among high-risk women. The annual cost burden of using adjunct ultrasound to screen high-risk women who cannot receive MRI in Ontario would be small.
Figures

Similar articles
-
Supplemental Screening as an Adjunct to Mammography for Breast Cancer Screening in People With Dense Breasts: A Health Technology Assessment.Ont Health Technol Assess Ser. 2023 Dec 19;23(9):1-293. eCollection 2023. Ont Health Technol Assess Ser. 2023. PMID: 39364436 Free PMC article.
-
Magnetic Resonance Imaging as an Adjunct to Mammography for Breast Cancer Screening in Women at Less Than High Risk for Breast Cancer: A Health Technology Assessment.Ont Health Technol Assess Ser. 2016 Nov 1;16(20):1-30. eCollection 2016. Ont Health Technol Assess Ser. 2016. PMID: 27990198 Free PMC article. Review.
-
Screening mammography for women aged 40 to 49 years at average risk for breast cancer: an evidence-based analysis.Ont Health Technol Assess Ser. 2007;7(1):1-32. Epub 2007 Jan 1. Ont Health Technol Assess Ser. 2007. PMID: 23074501 Free PMC article.
-
Cancer screening with digital mammography for women at average risk for breast cancer, magnetic resonance imaging (MRI) for women at high risk: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(3):1-55. Epub 2010 Mar 1. Ont Health Technol Assess Ser. 2010. PMID: 23074406 Free PMC article.
-
Performance of Screening Ultrasonography as an Adjunct to Screening Mammography in Women Across the Spectrum of Breast Cancer Risk.JAMA Intern Med. 2019 May 1;179(5):658-667. doi: 10.1001/jamainternmed.2018.8372. JAMA Intern Med. 2019. PMID: 30882843 Free PMC article.
Cited by
-
Ultrasound Imaging Technologies for Breast Cancer Detection and Management: A Review.Ultrasound Med Biol. 2018 Jan;44(1):37-70. doi: 10.1016/j.ultrasmedbio.2017.09.012. Epub 2017 Oct 26. Ultrasound Med Biol. 2018. PMID: 29107353 Free PMC article. Review.
-
How can additional ultrasonography screening improve the detection of occult breast cancer in women with dense breasts?Pol J Radiol. 2020 Jul 13;85:e353-e360. doi: 10.5114/pjr.2020.97944. eCollection 2020. Pol J Radiol. 2020. PMID: 32817768 Free PMC article.
-
Budget impact analysis of a breast rapid diagnostic unit.Curr Oncol. 2017 Jun;24(3):e214-e219. doi: 10.3747/co.24.3381. Epub 2017 Jun 27. Curr Oncol. 2017. PMID: 28680289 Free PMC article.
-
Diagnostic value of endoscopic ultrasound elastography for benign and malignant digestive system tumors.Pak J Med Sci. 2019 Sep-Oct;35(5):1461-1465. doi: 10.12669/pjms.35.5.1075. Pak J Med Sci. 2019. PMID: 31489026 Free PMC article.
-
Breast ultrasound in Chinese hospitals: A cross-sectional study of the current status and influencing factors of BI-RADS utilization and diagnostic accuracy.Lancet Reg Health West Pac. 2022 Aug 27;29:100576. doi: 10.1016/j.lanwpc.2022.100576. eCollection 2022 Dec. Lancet Reg Health West Pac. 2022. PMID: 36065174 Free PMC article.
References
-
- Canadian Cancer Society's Advisory Committee on Cancer Statistics. Canadian cancer statistics 2015. [Internet]. Toronto (On): Canadian Cancer Society; 2015. [cited 2015 Aug]. Available from: http://www.cancer.ca/statistics
-
- Erbas B, Provenzano E, Armes J, Gertig D. The natural history of ductal carcinoma in situ of the breast: a review. Breast Cancer Res Treat. 2006;97 (2): 135–44. - PubMed
-
- Narod SA, Iqbal J, Giannakeas V, Sopik V, Sun P. Breast cancer mortality after a diagnosis of ductal carcinoma in situ. JAMA Oncol. 2015;1 (7): 888–96. - PubMed
-
- Cancer Care Ontario. About the Ontario Breast Screening Program [Internet]. 2014. [cited 2015 May]. Available from: https://www.cancercare.on.ca/pcs/screening/breastscreening/obsp/
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous