

Single-Incision Carpal Tunnel Release and Distal Radius Open Reduction and Internal Fixation: A Cadaveric Study
- PMID: 27468377
- PMCID: PMC4959898
- DOI: 10.1055/s-0036-1581053
Single-Incision Carpal Tunnel Release and Distal Radius Open Reduction and Internal Fixation: A Cadaveric Study
Abstract
Background: The safety of surgical approaches for single- versus double-incision carpal tunnel release in association with distal radius open reduction and internal fixation remains controversial.
Purpose: The purpose of this study was to identify critical structures to determine if a single-incision extension of the standard flexor carpi radialis (FCR) approach can be performed safely.
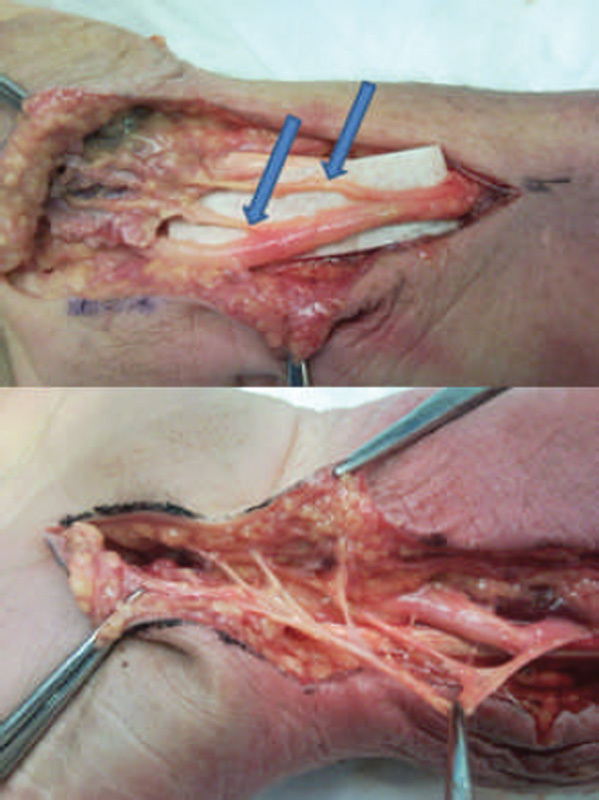
Methods: Nine cadaveric arms with were dissected under loupe magnification, utilizing a standard FCR approach. After the distal radius exposure was complete, the distal portion of the FCR incision was extended to allow release of the carpal tunnel. Dissection of critical structures was performed, including the recurrent thenar motor branch of the median nerve, the palmar cutaneous branch of the median nerve (PCBm), the palmar carpal and superficial palmar branches of the radial artery, and proximally the median nerve proper. The anatomic relationship of these structures relative to the surgical approach was recorded.
Results: Extension of the standard FCR approach as described in this study did not damage any critical structure in the specimens dissected. The PCBm was noted to arise from the radial side of the median nerve an average of 6.01cm proximal to the proximal edge of the transverse carpal ligament. The PCBm became enveloped in the layers of the antebrachial fascia and the transverse carpal ligament at the incision site, protecting it from injury. The recurrent motor branch of the median nerve, branches of the radial artery and the median nerve proper were not at risk during extension of the FCR approach to release the carpal tunnel.
Conclusions: Extension of the standard FCR approach to include carpal tunnel release can be performed with minimal risk to the underlying structures. This exposure may offer benefits in both visualization and extent of carpal tunnel release.
Keywords: acute carpal tunnel release; distal radius volar plating; extended flexor carpi radialis approach; motor recurrent; palmar cutaneous branch median nerve.
Conflict of interest statement
Figures





Similar articles
-
Single-incision extensile volar approach to the distal radius and concurrent carpal tunnel release: cadaveric study.J Hand Surg Am. 2010 Feb;35(2):217-22. doi: 10.1016/j.jhsa.2009.11.011. J Hand Surg Am. 2010. PMID: 20141892
-
Volar plate osteosynthesis of distal radius fractures with concurrent prophylactic carpal tunnel release using a hybrid flexor carpi radialis approach.J Hand Surg Am. 2010 Jul;35(7):1082-1088.e4. doi: 10.1016/j.jhsa.2010.03.043. J Hand Surg Am. 2010. PMID: 20610052
-
The Extended Flexor Carpi Radialis Approach for Concurrent Carpal Tunnel Release and Volar Plate Osteosynthesis for Distal Radius Fracture.J Hand Surg Am. 2015 Oct;40(10):2026-2031.e1. doi: 10.1016/j.jhsa.2015.07.001. Epub 2015 Aug 22. J Hand Surg Am. 2015. PMID: 26304737
-
Practical anatomy of the carpal tunnel.Hand Clin. 2002 May;18(2):219-30. doi: 10.1016/s0749-0712(01)00003-8. Hand Clin. 2002. PMID: 12371025 Review.
-
Anatomy of the palmar cutaneous branch of the median nerve: A review.J Orthop. 2019 Jun 5;16(6):576-579. doi: 10.1016/j.jor.2019.06.010. eCollection 2019 Nov-Dec. J Orthop. 2019. PMID: 31660025 Free PMC article. Review.
Cited by
-
Surgical Technique for Concurrent Endoscopic Carpal Tunnel Release and Distal Radius Fracture Fixation Using the Flexor Carpi Radialis Approach: A Case Series.J Hand Surg Glob Online. 2022 Jan 13;4(3):166-171. doi: 10.1016/j.jhsg.2021.11.007. eCollection 2022 May. J Hand Surg Glob Online. 2022. PMID: 35601523 Free PMC article.
-
Intraoperative Nerve Conduction Studies During Open Carpal Tunnel Release: A Pilot Study.Eplasty. 2022 Dec 7;22:e63. eCollection 2022. Eplasty. 2022. PMID: 36545639 Free PMC article.
-
Incidence of Carpal Tunnel Syndrome in Distal Radius Fractures Treated by Various Modalities in a Tertiary Care Center: A Single Center Study.Cureus. 2023 Feb 23;15(2):e35346. doi: 10.7759/cureus.35346. eCollection 2023 Feb. Cureus. 2023. PMID: 36974255 Free PMC article.
-
A Cadaveric Comparison of Approaches for Exposure of the Volar Distal Radius: Is There a Utilitarian Approach?Hand (N Y). 2024 Jan;19(1):44-51. doi: 10.1177/15589447221094320. Epub 2022 Jun 13. Hand (N Y). 2024. PMID: 35695337 Free PMC article.
-
Risk Assessment of Injury to Palmar Cutaneous Branch of the Median Nerve Using High-Resolution Ultrasound.Ann Rehabil Med. 2019 Aug;43(4):458-464. doi: 10.5535/arm.2019.43.4.458. Epub 2019 Aug 31. Ann Rehabil Med. 2019. PMID: 31499599 Free PMC article.
References
-
- Shauver M J, Yin H, Banerjee M, Chung K C. Current and future national costs to medicare for the treatment of distal radius fracture in the elderly. J Hand Surg Am. 2011;36(8):1282–1287. - PubMed
-
- Farner S, Malkani A, Lau E, Day J, Ochoa J, Ong K. Outcomes and cost of care for patients with distal radius fractures. Orthopedics. 2014;37(10):e866–e878. - PubMed
-
- Koval K J, Harrast J J, Anglen J O, Weinstein J N. Fractures of the distal part of the radius. The evolution of practice over time. Where's the evidence? J Bone Joint Surg Am. 2008;90(9):1855–1861. - PubMed
-
- Cooney W P III, Dobyns J H, Linscheid R L. Complications of Colles' fractures. J Bone Joint Surg Am. 1980;62(4):613–619. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
