

Obesity and Subtypes of Incident Cardiovascular Disease
- PMID: 27468925
- PMCID: PMC5015307
- DOI: 10.1161/JAHA.116.003921
Obesity and Subtypes of Incident Cardiovascular Disease
Abstract
Background: Obesity is a risk factor for various subtypes of cardiovascular disease (CVD), including coronary heart disease (CHD), heart failure (HF), and stroke. Nevertheless, there are limited comparisons of the associations of obesity with each of these CVD subtypes, particularly regarding the extent to which they are unexplained by traditional CVD mediators.
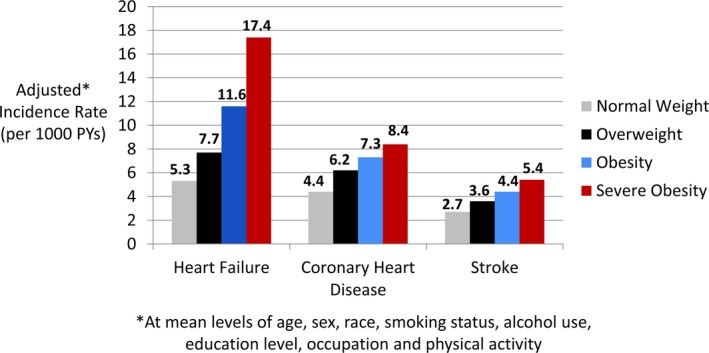
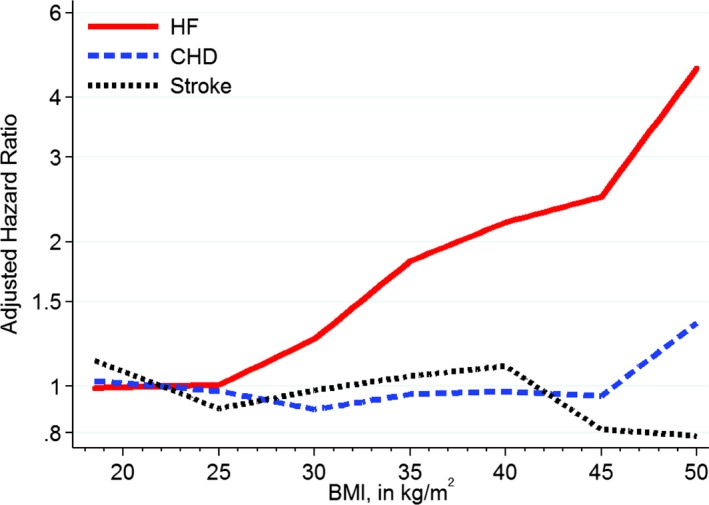
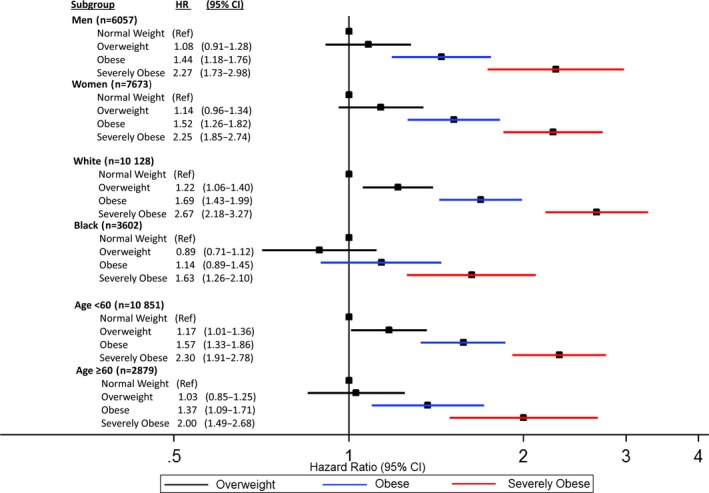
Methods and results: We followed 13 730 participants in the Atherosclerosis Risk in Communities (ARIC) study who had a body mass index ≥18.5 and no CVD at baseline (visit 1, 1987-1989). We compared the association of higher body mass index with incident HF, CHD, and stroke before and after adjusting for traditional CVD mediators (including systolic blood pressure, diabetes mellitus, and lipid measures). Over a median follow-up of 23 years, there were 2235 HF events, 1653 CHD events, and 986 strokes. After adjustment for demographics, smoking, physical activity, and alcohol intake, higher body mass index had the strongest association with incident HF among CVD subtypes, with hazard ratios for severe obesity (body mass index ≥35 versus normal weight) of 3.74 (95% CI 3.24-4.31) for HF, 2.00 (95% CI 1.67-2.40) for CHD, and 1.75 (95% CI 1.40-2.20) for stroke (P<0.0001 for comparisons of HF versus CHD or stroke). Further adjustment for traditional mediators fully explained the association of higher body mass index with CHD and stroke but not with HF (hazard ratio 2.27, 95% CI 1.94-2.64).
Conclusions: The link between obesity and HF was stronger than those for other CVD subtypes and was uniquely unexplained by traditional risk factors. Weight management is likely critical for optimal HF prevention, and nontraditional pathways linking obesity to HF need to be elucidated.
Keywords: coronary heart disease; epidemiology; heart failure; obesity; stroke.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Comment in
-
Editorial: The role of metabolic syndrome and disorders in cardiovascular disease.Front Endocrinol (Lausanne). 2023 Oct 31;14:1327394. doi: 10.3389/fendo.2023.1327394. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38027170 Free PMC article. No abstract available.
References
-
- Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi‐Sunyer FX, Eckel RH. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation. 2006;113:898–918. - PubMed
-
- Zalesin KC, Franklin BA, Miller WM, Peterson ED, McCullough PA. Impact of obesity on cardiovascular disease. Med Clin North Am. 2011;95:919–937. - PubMed
-
- Pandey A, Berry JD, Lavie CJ. Cardiometabolic disease leading to heart failure: better fat and fit than lean and lazy. Curr Heart Fail Rep. 2015;12:302–308. - PubMed
-
- Aune D, Sen A, Norat T, Janszky I, Romundstad P, Tonstad S, Vatten LJ. Body mass index, abdominal fatness, and heart failure incidence and mortality: a systematic review and dose‐response meta‐analysis of prospective studies. Circulation. 2016;133:639–649. - PubMed
-
- Davis MP, Rhode PC, Dutton GR, Redmann SM, Ryan DH, Brantley PJ. A primary care weight management intervention for low‐income African‐American women. Obesity (Silver Spring). 2006;14:1412–1420. - PubMed
Publication types
MeSH terms
Grants and funding
- K23 HL122447/HL/NHLBI NIH HHS/United States
- K24 DK106414/DK/NIDDK NIH HHS/United States
- L30 HL129418/HL/NHLBI NIH HHS/United States
- R01 DK089174/DK/NIDDK NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
