

Cumulative burden of cardiovascular morbidity in paediatric, adolescent, and young adult survivors of Hodgkin's lymphoma: an analysis from the St Jude Lifetime Cohort Study
- PMID: 27470081
- PMCID: PMC5029267
- DOI: 10.1016/S1470-2045(16)30215-7
Cumulative burden of cardiovascular morbidity in paediatric, adolescent, and young adult survivors of Hodgkin's lymphoma: an analysis from the St Jude Lifetime Cohort Study
Abstract
Background: The magnitude of cardiovascular morbidity in paediatric, adolescent, and young adult survivors of Hodgkin's lymphoma is not known. Using medically ascertained data, we applied the cumulative burden metric to compare chronic cardiovascular health conditions in survivors of Hodgkin's lymphoma and general population controls.
Methods: For this study, participant data were obtained from two ongoing cohort studies at St Jude Children's Research Hospital: the St Jude Lifetime Cohort Study (SJLIFE) and the St Jude Long-term Follow-up Study (SJLTFU). SJLIFE is a cohort study initiated on April 27, 2007, to enable longitudinal clinical evaluation of health outcomes of survivors of childhood cancer treated or followed at St Jude Children's Research Hospital, and SJLTFU is an administrative system-based study initiated in 2000 to collect outcome and late toxicity data for all patients treated at the hospital for childhood cancer. The patient cohort for our study was defined as patients treated at St Jude Children's Research Hospital who reached 18 years of age and were at least 10 years post-diagnosis of pathologically confirmed primary Hodgkin's lymphoma. Outcomes in the Hodgkin's lymphoma survivors were compared with a sample of SJLIFE community control participants, aged 18 years or older at the time of assessment, frequency-matched based on strata defined by 5-year age blocks within each sex, who were selected irrespective of previous medical history. All SJLIFE participants underwent assessment for 22 chronic cardiovascular health conditions. Direct assessments, combined with retrospective clinical reviews, were used to assign severity to conditions using a modified Common Terminology Criteria of Adverse Events (CTCAE) version 4.03 grading schema. Occurrences and CTCAE grades of the conditions for eligible non-SJLIFE participants were accounted for by multiple imputation. The mean cumulative count (treating death as a competing risk) was used to estimate cumulative burden.
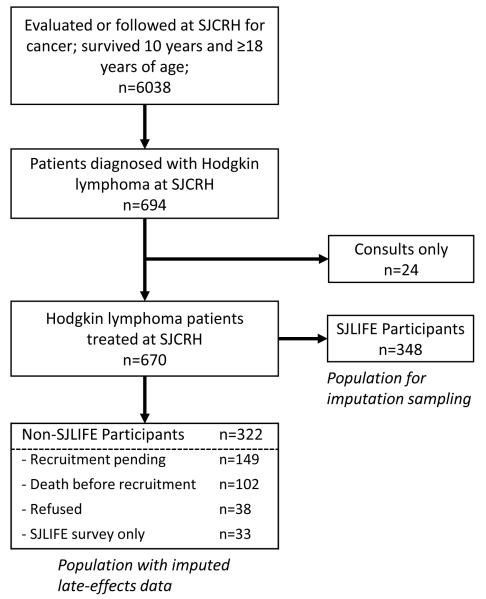
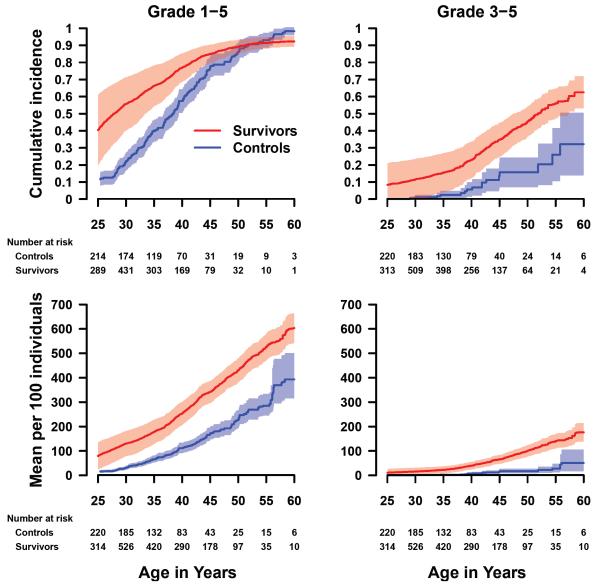
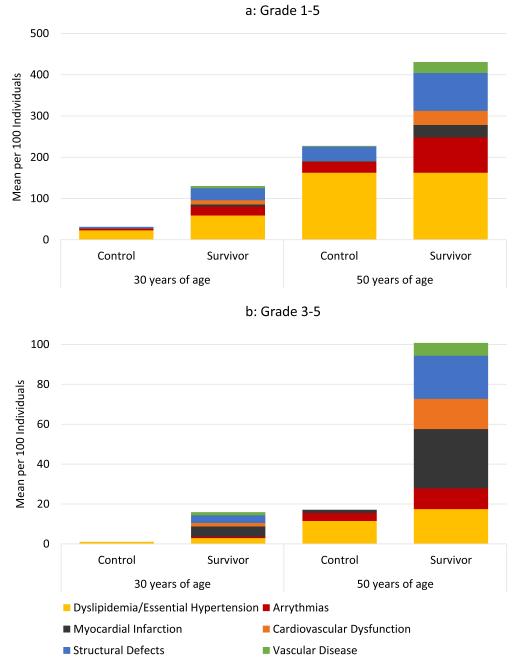
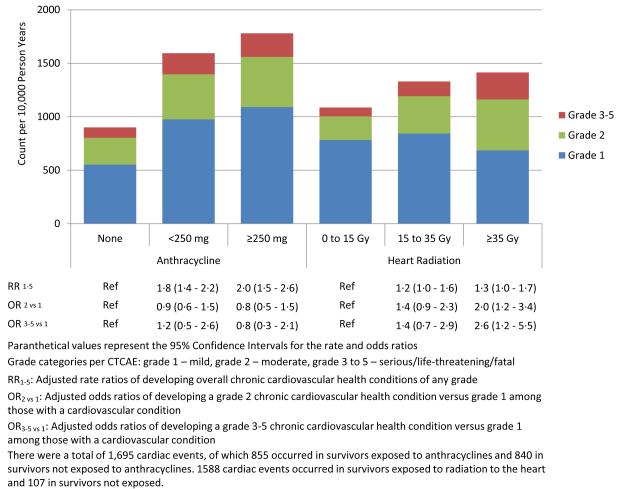
Findings: Of 670 survivors treated at St Jude Children's Research Hospital, who survived 10 years or longer and reached age 18 years, 348 were clinically assessed in the St Jude Lifetime Cohort Study (SJLIFE); 322 eligible participants did not participate in SJLIFE. Age and sex frequency-matched SJLIFE community controls (n=272) were used for comparison. At age 50 years, the cumulative incidence of survivors experiencing at least one grade 3-5 cardiovascular condition was 45·5% (95% CI 36·6-54·3), compared with 15·7% (7·0-24·4) in community controls. The survivor cohort at age 50 experienced a cumulative burden of 430·6 (95% CI 380·7-480·6) grade 1-5 and 100·8 (77·3-124·3) grade 3-5 cardiovascular conditions per 100 survivors; these numbers were appreciably higher than those in the control cohort (227·4 [192·7-267·5] grade 1-5 conditions and 17·0 [8·4-27·5] grade 3-5 conditions per 100 individuals). Myocardial infarction and structural heart defects were the major contributors to the excess grade 3-5 cumulative burden in survivors. High cardiac radiation dose (≥35 Gy) was associated with an increased proportion of grade 3-5 cardiovascular burden, whereas increased anthracyline dose was not.
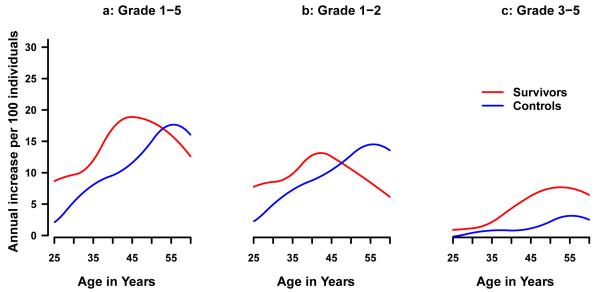
Interpretation: The true effect of cardiovascular morbidity in paediatric, adolescent, and young adult survivors of Hodgkin's lymphoma is reflected in the cumulative burden. Survivors aged 50 years will experience more than two times the number of chronic cardiovascular health conditions and nearly five times the number of more severe (grade 3-5) cardiovascular conditions compared with community controls and, on average, have one severe, life-threatening, or fatal cardiovascular condition. The cumulative burden metric provides a more comprehensive approach for assessing overall morbidity compared with currently used cumulative incidence based analytic methodologies, and will assist clinical researchers when designing future trials and refining general practice screening guidelines.
Funding: US National Cancer Institute, St Baldrick's Foundation, and American Lebanese Syrian Associated Charities.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Cumulative burden of disease: a relevant measure of the late side-effects of cancer treatment.Lancet Oncol. 2016 Sep;17(9):1189-90. doi: 10.1016/S1470-2045(16)30283-2. Epub 2016 Jul 25. Lancet Oncol. 2016. PMID: 27470082 No abstract available.
References
-
- US Department of Health and Human Services. National Cancer Institute Cancer Incidence and Survival among Children and Adolescents: United States SEER Program 1975-1995. 2013:1–192.
-
- Adams MJ, Lipsitz SR, Colan SD, et al. Cardiovascular status in long-term survivors of Hodgkin's disease treated with chest radiotherapy. J Clin Oncol. 2004;22:3139–48. - PubMed
-
- Galper SL, Yu JB, Mauch PM, et al. Clinically significant cardiac disease in patients with Hodgkin lymphoma treated with mediastinal irradiation. Blood. 2011;117:412–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
