

High attenuation areas on chest computed tomography in community-dwelling adults: the MESA study
- PMID: 27471206
- PMCID: PMC5089905
- DOI: 10.1183/13993003.00129-2016
High attenuation areas on chest computed tomography in community-dwelling adults: the MESA study
Abstract
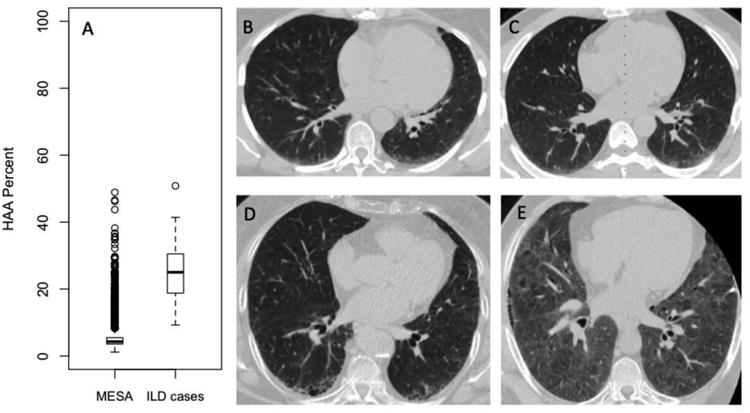
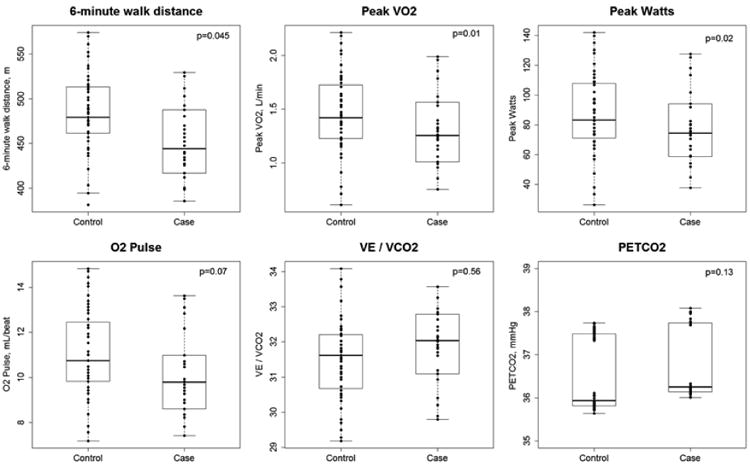
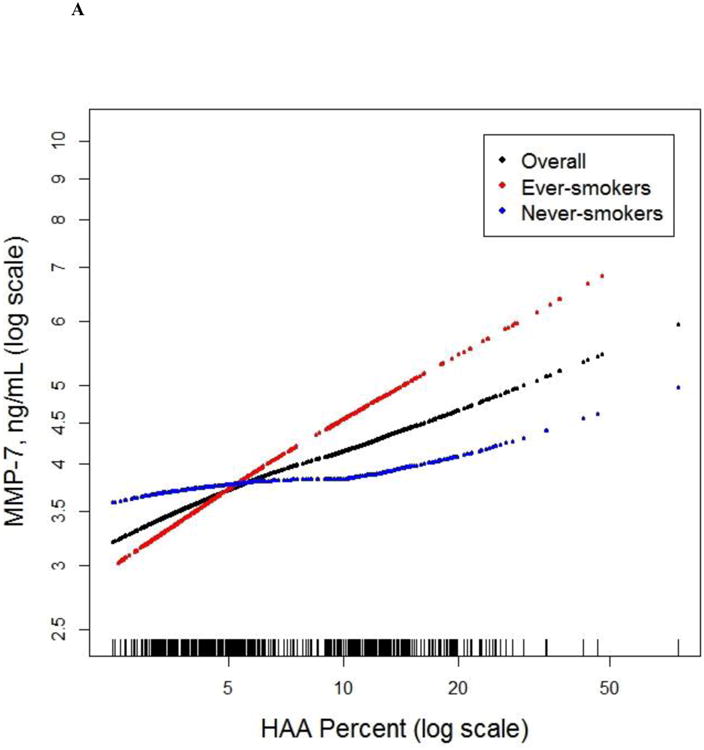
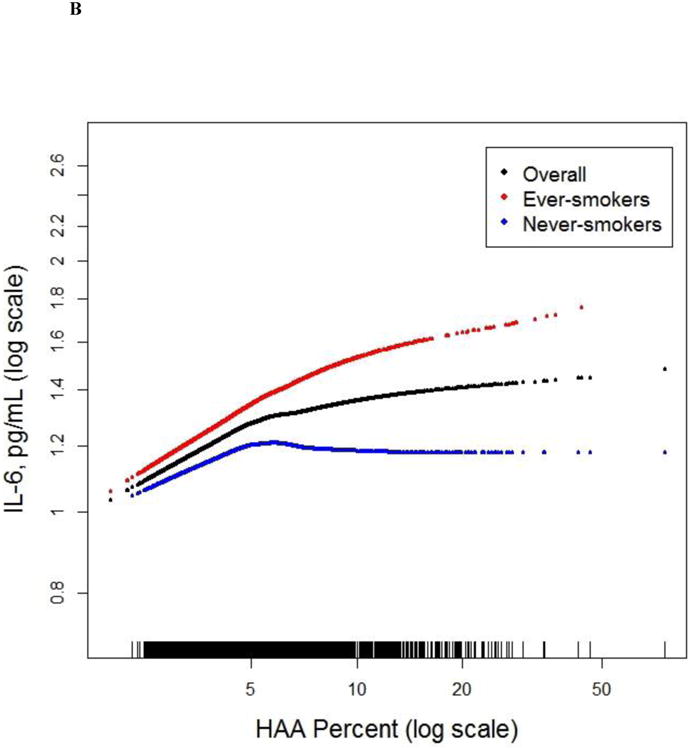
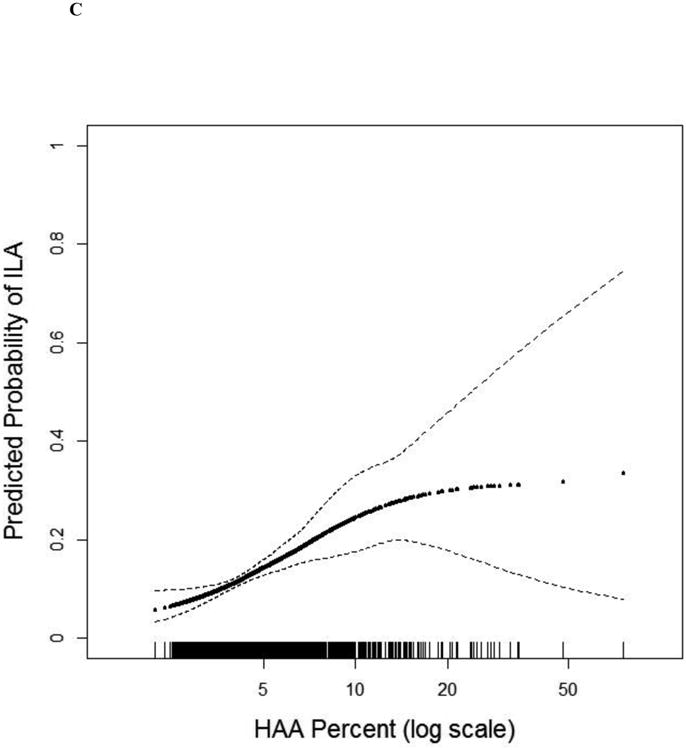
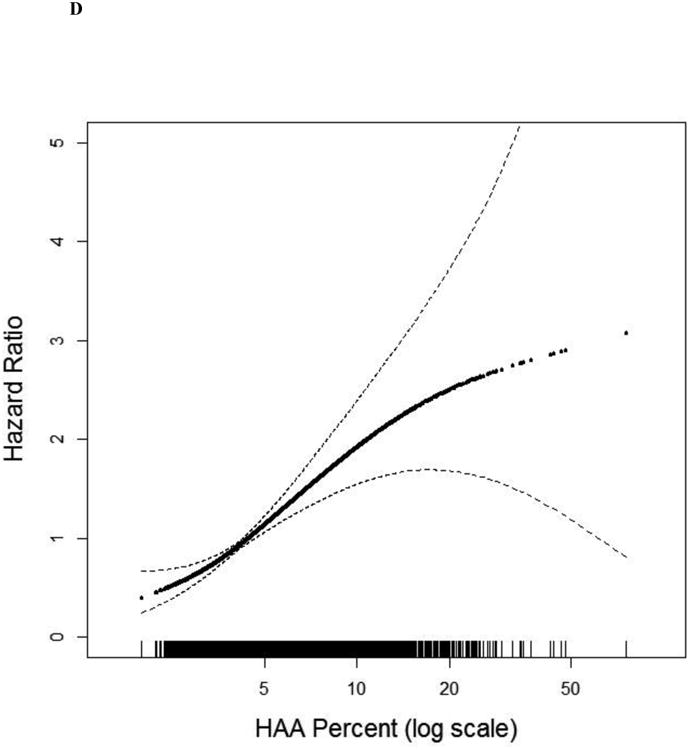
Evidence suggests that lung injury, inflammation and extracellular matrix remodelling precede lung fibrosis in interstitial lung disease (ILD). We examined whether a quantitative measure of increased lung attenuation on computed tomography (CT) detects lung injury, inflammation and extracellular matrix remodelling in community-dwelling adults sampled without regard to respiratory symptoms or smoking.We measured high attenuation areas (HAA; percentage of lung voxels between -600 and -250 Hounsfield Units) on cardiac CT scans of adults enrolled in the Multi-Ethnic Study of Atherosclerosis.HAA was associated with higher serum matrix metalloproteinase-7 (mean adjusted difference 6.3% per HAA doubling, 95% CI 1.3-11.5), higher interleukin-6 (mean adjusted difference 8.8%, 95% CI 4.8-13.0), lower forced vital capacity (FVC) (mean adjusted difference -82 mL, 95% CI -119--44), lower 6-min walk distance (mean adjusted difference -40 m, 95% CI -1--80), higher odds of interstitial lung abnormalities at 9.5 years (adjusted OR 1.95, 95% CI 1.43-2.65), and higher all cause-mortality rate over 12.2 years (HR 1.58, 95% CI 1.39-1.79).High attenuation areas are associated with biomarkers of inflammation and extracellular matrix remodelling, reduced lung function, interstitial lung abnormalities, and a higher risk of death among community-dwelling adults.
Copyright ©ERS 2016.
Figures
Comment in
-
Imaging and molecular biomarkers: a novel approach to screen populations at risk of pulmonary fibrosis?Eur Respir J. 2016 Nov;48(5):1271-1273. doi: 10.1183/13993003.01673-2016. Eur Respir J. 2016. PMID: 27799380 No abstract available.
References
-
- Selman M, Pardo A. Alveolar epithelial cell disintegrity and subsequent activation: a key process in pulmonary fibrosis. Am J Respir Crit Care Med. 2012;186(2):119–121. - PubMed
-
- Kropski JA, Pritchett JM, Zoz DF, Crossno PF, Markin C, Garnett ET, Degryse AL, Mitchell DB, Polosukhin VV, Rickman OB, Choi L, Cheng DS, McConaha ME, Jones BR, Gleaves LA, McMahon FB, Worrell JA, Solus JF, Ware LB, Lee JW, Massion PP, Zaynagetdinov R, White ES, Kurtis JD, Johnson JE, Groshong SD, Lancaster LH, Young LR, Steele MP, Phillips JA, Iii, Cogan JD, Loyd JE, Lawson WE, Blackwell TS. Extensive Phenotyping of Individuals At-risk for Familial Interstitial Pneumonia Reveals Clues to the Pathogenesis of Interstitial Lung Disease. Am J Respir Crit Care Med. 2014 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- T32 HL105323/HL/NHLBI NIH HHS/United States
- N01 HC095164/HC/NHLBI NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- K23 HL083091/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- N01 HC095165/HC/NHLBI NIH HHS/United States
- N01 HC095168/HC/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- N01 HC095167/HC/NHLBI NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- R01 HL112986/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- N01 HC095161/HC/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- RC1 HL100543/HL/NHLBI NIH HHS/United States
- N01 HC095166/HC/NHLBI NIH HHS/United States
- N01 HC095160/HC/NHLBI NIH HHS/United States
- R01 HL114626/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01 HC095169/HC/NHLBI NIH HHS/United States
- U01 DK048443/DK/NIDDK NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095163/HC/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- K24 HL131937/HL/NHLBI NIH HHS/United States
- R01 HL103676/HL/NHLBI NIH HHS/United States
- K23 HL130627/HL/NHLBI NIH HHS/United States
- N01 HC095162/HC/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- K24 HL103844/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical