

Interactions between kidney disease and diabetes: dangerous liaisons
- PMID: 27471550
- PMCID: PMC4964290
- DOI: 10.1186/s13098-016-0159-z
Interactions between kidney disease and diabetes: dangerous liaisons
Abstract
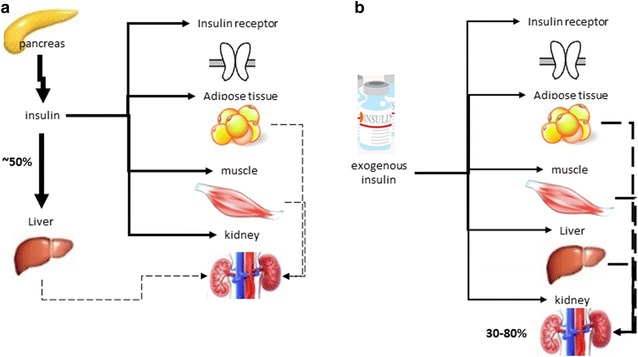
Background: Type 2 diabetes mellitus (DM) globally affects 18-20 % of adults over the age of 65 years. Diabetic kidney disease (DKD) is one of the most frequent and dangerous complications of DM2, affecting about one-third of the patients with DM2. In addition to the pancreas, adipocytes, liver, and intestines, the kidneys also play an important role in glycemic control, particularly due to renal contribution to gluconeogenesis and tubular reabsorption of glucose.
Methods: In this review article, based on a report of discussions from an interdisciplinary group of experts in the areas of endocrinology, diabetology and nephrology, we detail the relationship between diabetes and kidney disease, addressing the care in the diagnosis, the difficulties in achieving glycemic control and possible treatments that can be applied according to the different degrees of impairment.
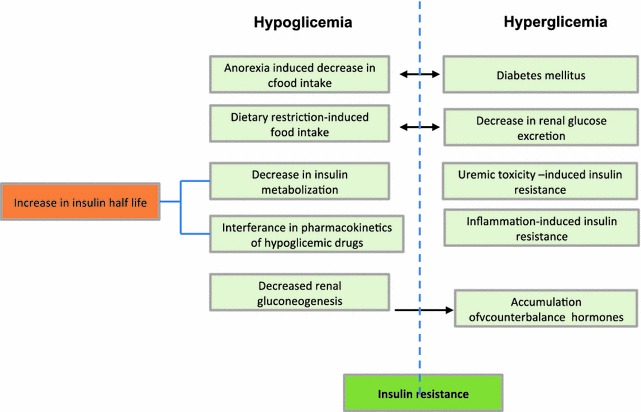
Discussion: Glucose homeostasis is extremely altered in patients with DKD, who are exposed to a high risk of both hyperglycemia and hypoglycemia. Both high and low glycemic levels are associated with increased morbidity and shortened survival in this group of patients. Factors that are associated with an increased risk of hypoglycemia in DKD patients include decreased renal gluconeogenesis, deranged metabolic pathways (including altered metabolism of medications) and decreased insulin clearance. On the other hand, decrease glucose filtration and excretion, and inflammation-induce insulin resistance are predisposing factors to hyperglycemic episodes.
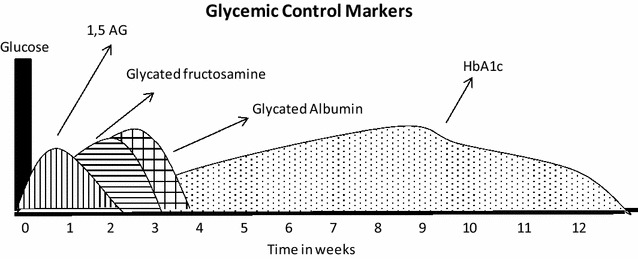
Conclusion: Appropriate glycaemic monitoring and control tailored for diabetic patients is required to avoid hypoglycaemia and other glycaemic disarrays in patients with DM2 and kidney disease. Understanding the renal physiology and pathophysiology of DKD has become essential to all specialties treating diabetic patients. Disseminating this knowledge and detailing the evidence will be important to initiate breakthrough research and to encourage proper treatment of this group of patients.
Keywords: Diabetes complications; Diabetic kidney disease; Glycemic control; Type 2 diabetes.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
