

Treatment efficacy of anti-hypertensive drugs in monotherapy or combination: ATOM systematic review and meta-analysis of randomized clinical trials according to PRISMA statement
- PMID: 27472680
- PMCID: PMC5265817
- DOI: 10.1097/MD.0000000000004071
Treatment efficacy of anti-hypertensive drugs in monotherapy or combination: ATOM systematic review and meta-analysis of randomized clinical trials according to PRISMA statement
Abstract
Background: The relative efficacy of antihypertensive drugs/combinations is not well known. Identifying the most effective ones and the patients' characteristics associated with best performance of the drugs will improve management of hypertensive patients.
Objective: To assess the blood pressure (BP) reduction attributed to antihypertensive drugs and identify characteristics associated with BP decrease.
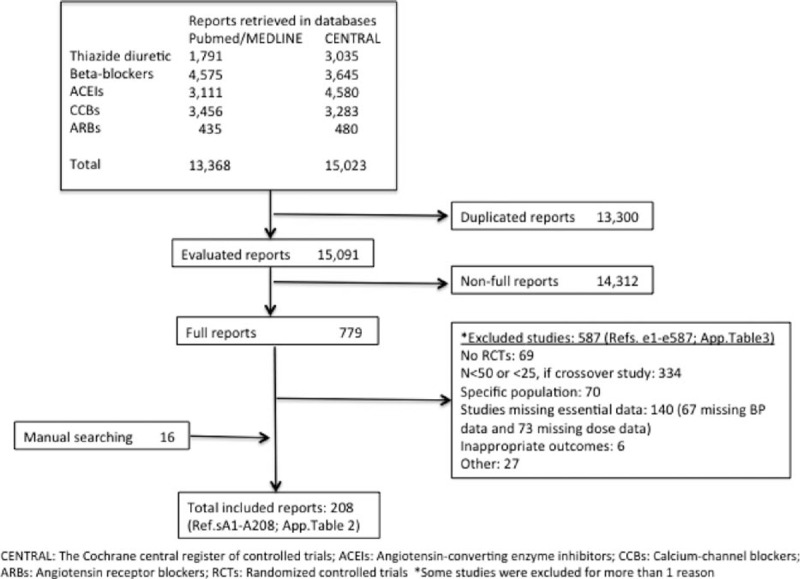
Data sources: MEDLINE, Cochrane Central Register of Controlled Trials from inception through July 2012 and selected papers.
Study eligibility criteria: Double-blind, randomized clinical trials whose main result was the reduction in BP by antihypertensive treatment, with study population ≥50 or ≥25 if the study was a crossover, follow-up of at least 8 weeks, and available required data.
Study appraisal and synthesis methods: Study data were independently extracted by multiple observers and introduced in an electronic database. Inconsistencies were resolved by discussion and referral back to the original articles. Meta-analysis was performed according to PRISMA statement and using a Bayesian framework.
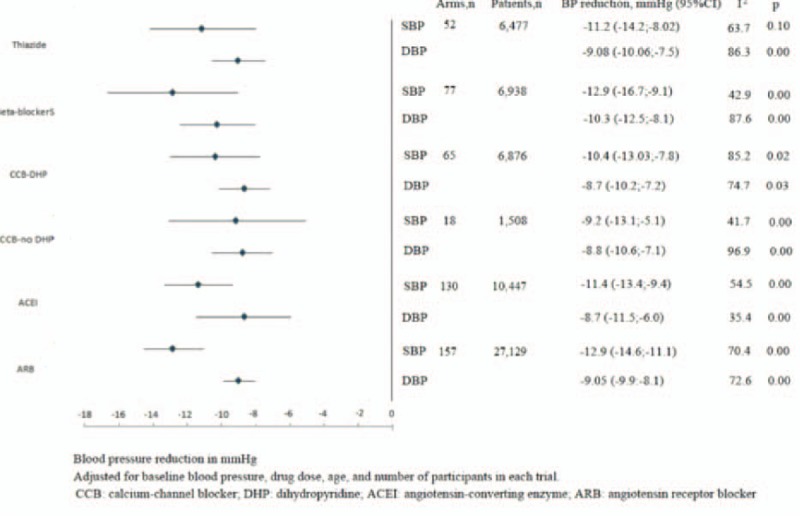
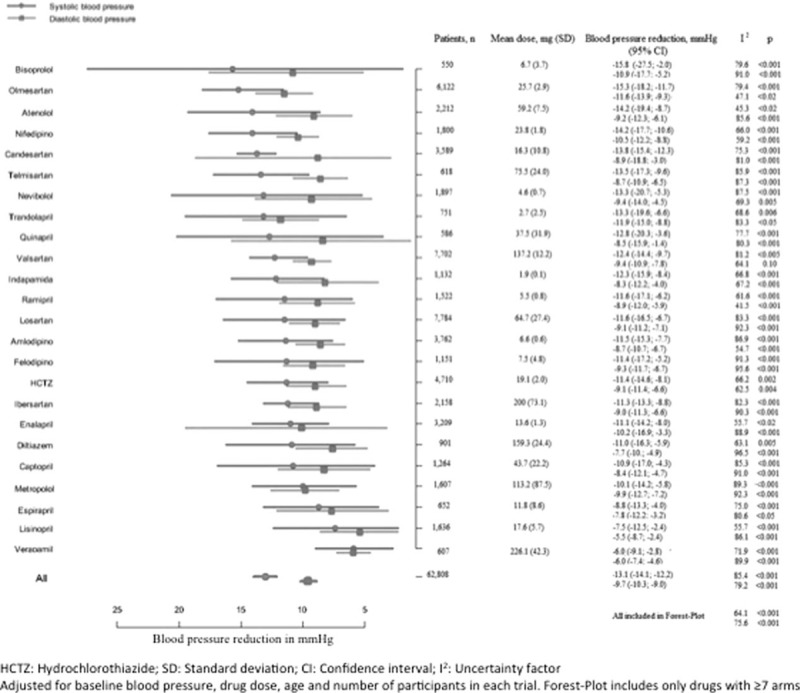
Main outcome(s) and measure(s): Mean decrease in systolic (SBP) and diastolic blood pressure (DBP) achieved by each drug or combination.
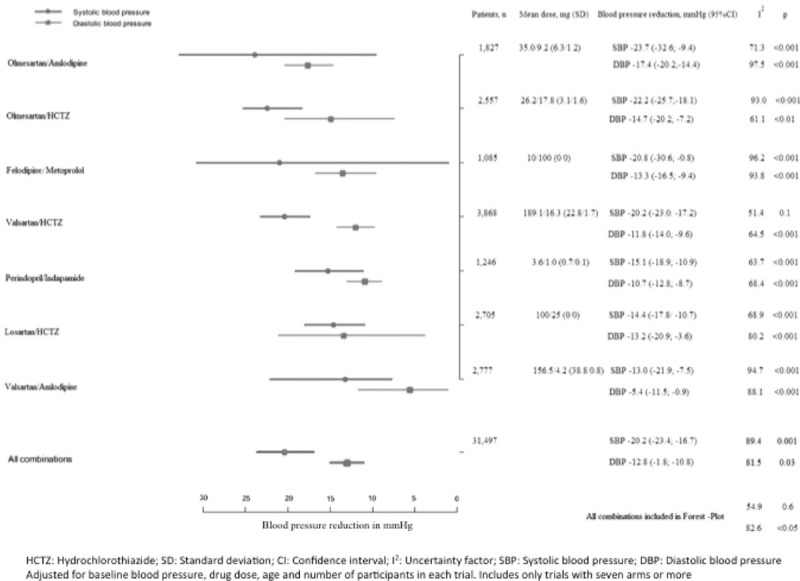
Results: Two hundred eight trials including 94,305 patients were identified. In monotherapy, most drugs achieved 10 to 15 mm Hg SBP and 8 to 10 mm Hg DBP decreases.Olmesartan/amlodipine, olmesartan/hydrochlorothiazide, felodipine/metoprolol, and valsartan/hydrochlorothiazide were the combinations leading to the greatest mean SBP reductions (>20 mm Hg). Female sex and body mass index >25 kg/m were associated with more pronounced SBP and DBP reductions, whereas Afro-American ethnicity was associated with BP reductions smaller than the median. Results were adjusted by study duration, cardiovascular disease, and diabetes mellitus. Still, the estimation was performed using the mean administered doses, which do not exactly match those of the available drug formats.
Limitations: Data corresponded to those obtained in each of the included trials; the analysis of the combinations was limited to the most recent ones; estimations were performed using the mean administered doses.
Conclusions and implications: Certain drug combinations achieve BP reductions ranging from 20 to 25/10 to 15 mm Hg. Sex, ethnicity, and obesity are associated with antihypertensive response. This information can contribute to better selection of the antihypertensive drug, depending on the magnitude of pretreatment BP elevation. Guidelines should be revised.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- ESH/ESC Task Force for the Management of Arterial Hypertension. Practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J Hypertens 2013; 31:1925–1938. - PubMed
-
- Materson BJ. Variability in response to antihypertensive drugs. Am J Med 2007; 120 (4 Suppl 1):S10–20. - PubMed
-
- Campo C, Segura J, Guerrero L, et al. Predictors of systolic blood pressure control with antihypertensive monotherapy [abstract]. J Hypertens 2000; 18 suppl 4:S41.
-
- Gupta AK, Poulter NR, Dobson J, et al. Ethnic differences in blood pressure response to first and second-line antihypertensive therapies in patients randomized in the ASCOT trial. Am J Hypertens 2010; 23:1023–1030. - PubMed
-
- Agarwal R, Weir MR. Blood pressure response with fixed-dose combination therapy: comparing hydrochlorothiazide with amlodipine through individual-level meta analysis. J Hypertens 2013; 31:1692–1701. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
