

Positron emission tomography and computed tomography angiography for the diagnosis of giant cell arteritis: A real-life prospective study
- PMID: 27472684
- PMCID: PMC5265821
- DOI: 10.1097/MD.0000000000004146
Positron emission tomography and computed tomography angiography for the diagnosis of giant cell arteritis: A real-life prospective study
Abstract
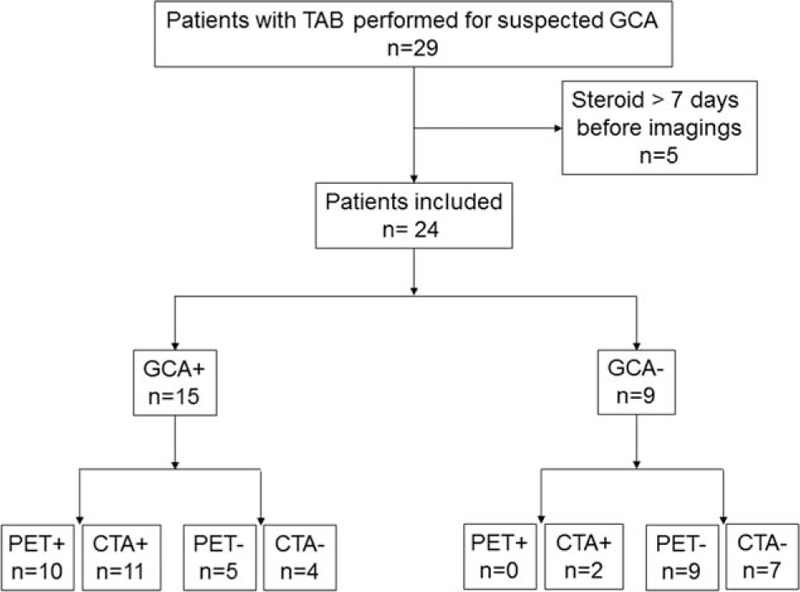
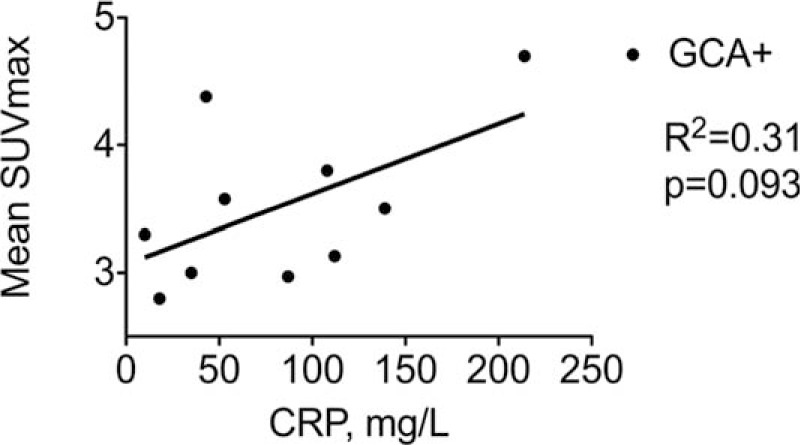
The use of 18F-fluoro-deoxyglucose positron emission tomography scan (FDG-PET) and computed tomography angiography (CTA) to improve accuracy of diagnosis of giant cell arteritis (GCA) is a very important clinical need. We aimed to compare the diagnostic performance of FDG-PET and CTA in patients with GCA.FDG-PET and CTA were acquired in all consecutive patients suspected for GCA. Results of FDG-PET and CTA were compared with the final diagnosis based on clinical judgment, temporal artery biopsy (TAB) findings, and ACR criteria. Sensitivity, specificity, and positive and negative predictive values (PPV, NPV) were calculated for each method.Twenty-four patients suspected for GCA were included. Fifteen (62.5%) were ultimately diagnosed as having GCA. Among them, all fulfilled ACR criteria and 6 had biopsy-proven GCA. Strong FDG uptake in large vessels was found in 10 patients who all had GCA. Mean maximal standard uptake values (SUVmax) per patient measured at all the arterial territories were of 3.7 (range: 2.8-4.7). FDG uptake was negative in 14 patients including 9 and 5 patients without and with GCA, respectively. Mural thickening suggestive of aortitis or branch vessel arteritis was observed on CTA in 11 patients with and 2 patients without GCA. No mural thickening was observed in 11 patients including 7 patients without and 4 patients with GCA. Overall, sensitivity was 66.7% and 73.3%, specificity was 100% and 84.6%, NPV was 64.3% and 64.6%, and PPV was 100% and 84.6% of FDG-PET and CTA, respectively.Both FDG-PET and CTA have a strong diagnostic yield for the diagnosis of GCA. FDG-PET appeared to have a higher PPV as compared to CTA and may be the preferred noninvasive technique to explore patients with suspected GCA.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Hunder GG, Bloch DA, Michel BA, et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum 1990; 33:1122–1128. - PubMed
-
- Rao JK, Allen NB, Pincus T. Limitations of the 1990 American College of Rheumatology classification criteria in the diagnosis of vasculitis. Ann Intern Med 1998; 129:345–352. - PubMed
-
- Blockmans D. Diagnosis and extension of giant cell arteritis. Contribution of imaging techniques. Presse Med 2012; 41:948–954. - PubMed
-
- Besson FL, Parienti JJ, Bienvenu B, et al. Diagnostic performance of (1)(8)F-fluorodeoxyglucose positron emission tomography in giant cell arteritis: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging 2011; 38:1764–1772. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
