

Metabolomic Profiling Identifies Novel Circulating Biomarkers of Mitochondrial Dysfunction Differentially Elevated in Heart Failure With Preserved Versus Reduced Ejection Fraction: Evidence for Shared Metabolic Impairments in Clinical Heart Failure
- PMID: 27473038
- PMCID: PMC5015273
- DOI: 10.1161/JAHA.115.003190
Metabolomic Profiling Identifies Novel Circulating Biomarkers of Mitochondrial Dysfunction Differentially Elevated in Heart Failure With Preserved Versus Reduced Ejection Fraction: Evidence for Shared Metabolic Impairments in Clinical Heart Failure
Abstract
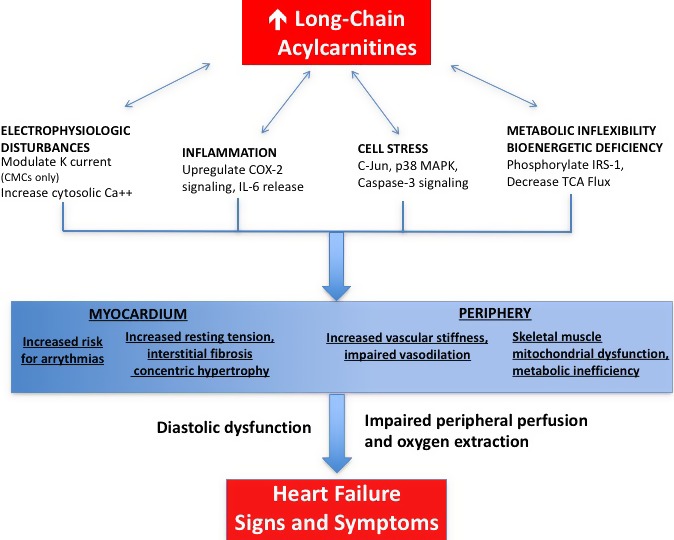
Background: Metabolic impairment is an important contributor to heart failure (HF) pathogenesis and progression. Dysregulated metabolic pathways remain poorly characterized in patients with HF and preserved ejection fraction (HFpEF). We sought to determine metabolic abnormalities in HFpEF and identify pathways differentially altered in HFpEF versus HF with reduced ejection fraction (HFrEF).
Methods and results: We identified HFpEF cases, HFrEF controls, and no-HF controls from the CATHGEN study of sequential patients undergoing cardiac catheterization. HFpEF cases (N=282) were defined by left ventricular ejection fraction (LVEF) ≥45%, diastolic dysfunction grade ≥1, and history of HF; HFrEF controls (N=279) were defined similarly, except for having LVEF <45%. No-HF controls (N=191) had LVEF ≥45%, normal diastolic function, and no HF diagnosis. Targeted mass spectrometry and enzymatic assays were used to quantify 63 metabolites in fasting plasma. Principal components analysis reduced the 63 metabolites to uncorrelated factors, which were compared across groups using ANCOVA. In basic and fully adjusted models, long-chain acylcarnitine factor levels differed significantly across groups (P<0.0001) and were greater in HFrEF than HFpEF (P=0.0004), both of which were greater than no-HF controls. We confirmed these findings in sensitivity analyses using stricter inclusion criteria, alternative LVEF thresholds, and adjustment for insulin resistance.
Conclusions: We identified novel circulating metabolites reflecting impaired or dysregulated fatty acid oxidation that are independently associated with HF and differentially elevated in HFpEF and HFrEF. These results elucidate a specific metabolic pathway in HF and suggest a shared metabolic mechanism in HF along the LVEF spectrum.
Keywords: fatty acid oxidation; heart failure; metabolism; metabolomics; mitochondrial dysfunction.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Després JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER III, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB; American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Executive summary: heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131:434–441. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Hogg K, Swedberg K, McMurray J. Heart failure with preserved left ventricular systolic function; epidemiology, clinical characteristics, and prognosis. J Am Coll Cardiol. 2004;43:317–327. - PubMed
-
- Steinberg BA, Zhao X, Heidenreich PA, Peterson ED, Bhatt DL, Cannon CP, Hernandez AF, Fonarow GC; Get With the Guidelines Scientific Advisory Committee and Investigators . Trends in patients hospitalized with heart failure and preserved left ventricular ejection fraction: prevalence, therapies, and outcomes. Circulation. 2012;126:65–75. - PubMed
-
- Senni M, Redfield MM. Heart failure with preserved systolic function: a different natural history? J Am Coll Cardiol. 2001;38:1277–1282. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
