

ROHHAD syndrome and evolution of sleep disordered breathing
- PMID: 27473663
- PMCID: PMC4967322
- DOI: 10.1186/s13023-016-0484-1
ROHHAD syndrome and evolution of sleep disordered breathing
Abstract
Background: Rapid-onset obesity with hypothalamic dysfunction, hypoventilation and autonomic dysregulation (ROHHAD) is a rare disease with a high mortality rate. Although nocturnal hypoventilation (NH) is central to ROHHAD, the evolution of sleep disordered breathing (SDB) is not well studied. The aim of the study was to assess early manifestations of SDB and their evolution in ROHHAD syndrome.
Methods: Retrospective study of children with ROHHAD at two Canadian centers. All children with suspected ROHHAD at presentation underwent polysomnography (PSG) to screen for nocturnal hypoventilation. PSG findings at baseline and follow-up were collected. Interventions and diagnostic test results were recorded.
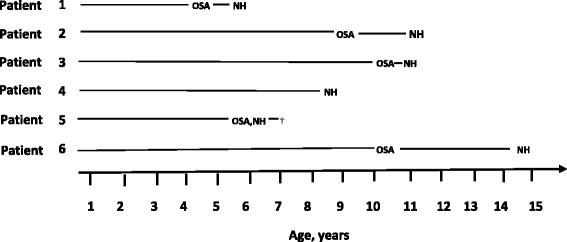
Results: Six children were included. The median age of rapid onset obesity and nocturnal hypoventilation (NH) was 3.5 and 7.2 years respectively. On initial screening for ROHHAD 4/6 (66.7 %) children had obstructive sleep apnea (OSA), 1/6 (16.7 %) had NH and 1/6 (16.7 %) had both OSA and NH. Follow up PSGs were performed in 5/6 children as one child died following a cardiorespiratory arrest. All children at follow up had NH and required non-invasive positive pressure ventilation. Additionally, 3/6 (50 %) children demonstrated irregular breathing patterns during wakefulness.
Conclusions: Children with ROHHAD may initially present with OSA and only develop NH later as well as dysregulation of breathing during wakefulness. The recognition of the spectrum of respiratory abnormalities at presentation and over time may be important in raising the index of suspicion of ROHHAD. Early recognition and targeted therapeutic interventions may limit morbidity and mortality associated with ROHHAD.
Keywords: Nocturnal hypoventilation; Polysomnogram; ROHHAD syndrome; Sleep disordered breathing.
Figures
References
-
- Bougneres P, Pantalone L, Linglart A, Rothenbuhler A, Le Stunff C. Endocrine manifestations of the rapid-onset obesity with hypoventilation, hypothalamic, autonomic dysregulation, and neural tumor syndrome in childhood. J Clin Endocrinol Metab. 2008;93:3971–80. doi: 10.1210/jc.2008-0238. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
