

Brain metastasis in lung cancer: Building a molecular and systems-level understanding to improve outcomes
- PMID: 27474492
- PMCID: PMC6020150
- DOI: 10.1016/j.biocel.2016.07.025
Brain metastasis in lung cancer: Building a molecular and systems-level understanding to improve outcomes
Abstract
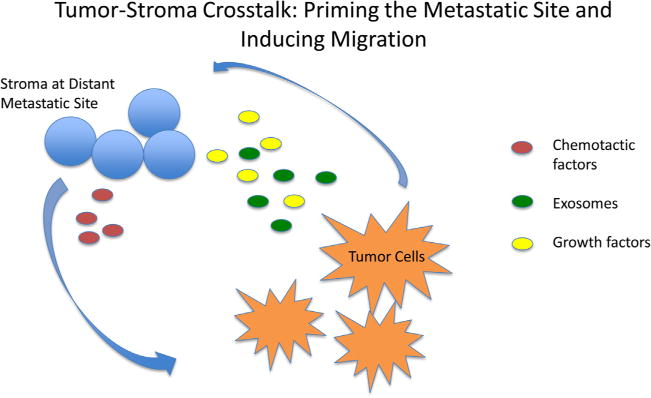
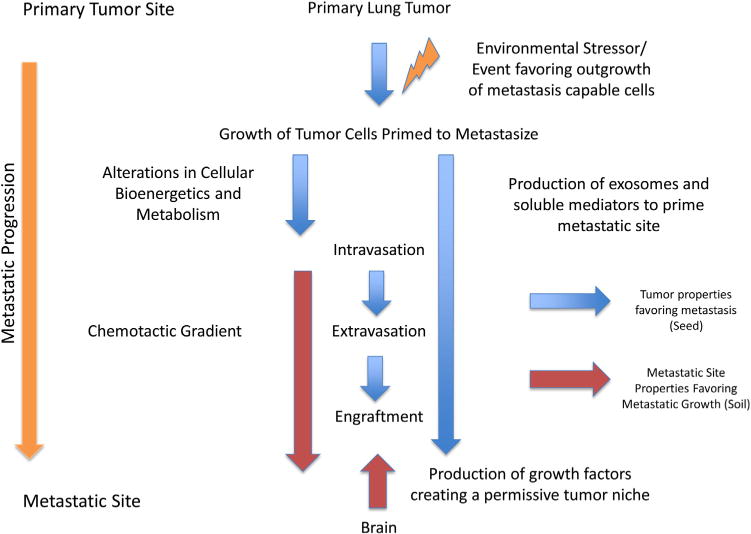
Lung cancer is a clinically difficult disease with rising disease burden around the world. Unfortunately, most lung cancers present at a clinically advanced stage. Of these cancers, many also present with brain metastasis which complicates the clinical picture. This review summarizes current knowledge on the molecular basis of lung cancer brain metastases. We start from the clinical perspective, aiming to provide a clinical context for a significant problem that requires much deeper scientific investigation. We review new research governing the metastatic process, including tumor cell signaling, establishment of a receptive tumor niches in the brain and evaluate potential new therapeutic options that take advantage of these new scientific advances. Lung cancer remains the largest single cause of cancer mortality in the United States (Siegel et al., 2015). This continues to be the clinical picture despite significant advances in therapy, including the advent of targeted molecular therapies and newly adopted immunotherapies for certain subtypes of lung cancer. In the vast majority of cases, lung cancer presents as advanced disease; in many instances, this advanced disease state is intimately associated with micro and macrometastatic disease (Goldberg et al., 2015). For both non-small cell lung cancer and small cell lung cancer patients, the predominant metastatic site is the brain, with up to 68% of patients with mediastinal lymph node metastasis eventually demonstrating brain metastasis (Wang et al., 2009).The frequency (incidence) of brain metastasis is highest in lung cancers, relative to other common epithelial malignancies (Schouten et al., 2002). Other studies have attempted to predict the risk of brain metastasis in the setting of previously non-metastatic disease. One of the largest studies to do this, analyzing historical data from 1973 to 2011 using the SEER database revealed a 9% risk of patients with previously non-metastatic NSCLC developing brain metastasis over the course of their disease, while 18% of small cell lung cancer patients without previous metastasis went on to develop brain metastasis as their disease progressed (Goncalves et al., 2016).The reasons underlying this predilection for the central nervous system, as well as the recent increase in the frequency of brain metastasis identified in patients remain important questions for both clinicians and basic scientists. More than ever, the question of how brain metastasis develop and how they can be treated and managed requires the involvement of interdisciplinary teams-and more importantly-scientists who are capable of thinking like clinicians and clinicians who are capable of thinking like scientists. This review aims to present a translational perspective on brain metastasis. We will investigate the scope of the problem of brain metastasis and the current management of the metastatic disease process in lung cancer. From this clinical starting point, we will investigate the literature surrounding the molecular underpinnings of lung tumor metastasis and seek to understand the process from a biological perspective to generate new hypotheses.
Keywords: Brain metastasis of lung cancer; Lung cancer; Metastasis; Non-small cell lung cancer; Small cell lung cancer.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
References
-
- Auperin A, et al. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission: prophylactic Cranial Irradiation Overview Collaborative Group. N Engl J Med. 1999;341(7):476–484. - PubMed
-
- Baykara M, et al. Management of brain metastases from non-small cell lung cancer. J Cancer Res Ther. 2014;10(4):915–921. - PubMed
-
- Bowden G, et al. Gamma knife radiosurgery for the management of cerebral metastases from non-small cell lung cancer. J Neurosurg. 2015;122(4):766–772. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
