

The Role of Acute Kidney Injury in Chronic Kidney Disease
- PMID: 27475659
- PMCID: PMC4979984
- DOI: 10.1016/j.semnephrol.2016.05.005
The Role of Acute Kidney Injury in Chronic Kidney Disease
Abstract
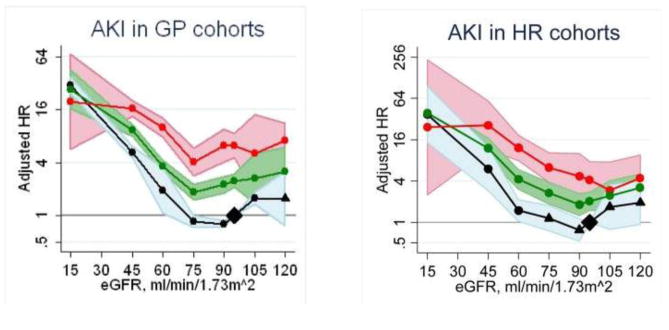
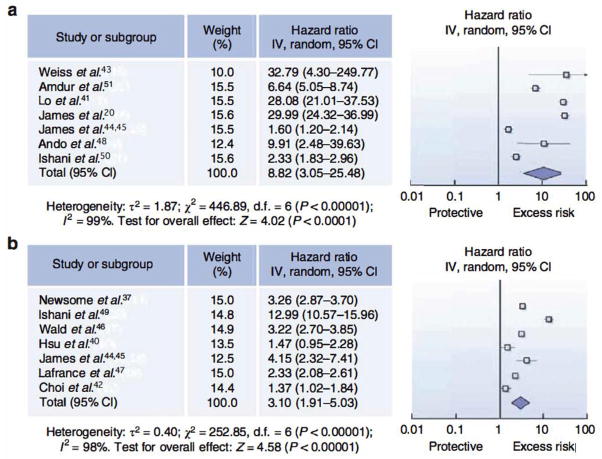
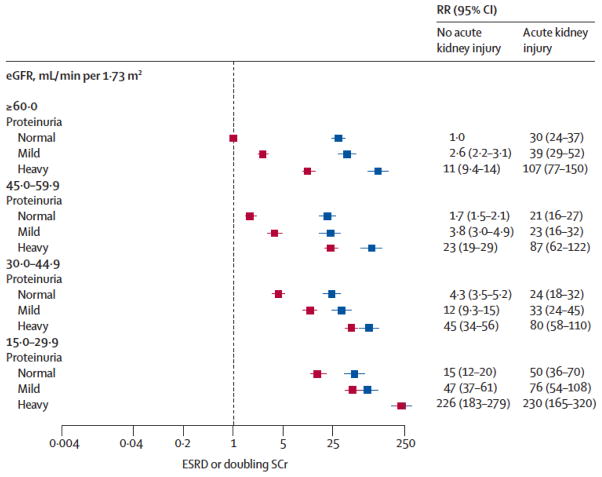
There is increasing recognition that acute kidney injury (AKI) and chronic kidney disease (CKD) are closely linked and likely promote one another. Underlying CKD now is recognized as a clear risk factor for AKI because both decreased glomerular filtration rate and increased proteinuria have been shown to be associated strongly with AKI. A growing body of literature also provides evidence that AKI accelerates the progression of CKD. Individuals who suffered dialysis-requiring AKI are particularly vulnerable to worse long-term renal outcomes, including end-stage renal disease. The association between AKI and subsequent renal function decline is amplified by pre-existing severity of CKD, higher stage of AKI, and the cumulative number of AKI episodes. However, residual confounding and ascertainment bias may partly explain the epidemiologic association between AKI and CKD in observational studies. As the number of AKI survivors increases, we need to better understand other clinically important outcomes after AKI, identify those at highest risk for the most adverse sequelae, and develop strategies to optimize their care.
Keywords: Acute kidney injury; acute renal failure; chronic kidney disease; epidemiology; outcomes.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- National Kidney Foundation. K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–S266. - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108(17):2154–2169. - PubMed
-
- Go A, Chertow G, Fan D, MuCulloch C, Hsu C. Chronic kidney disease and risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
-
- Hemmelgarn BR, Manns BJ, Lloyd A, et al. Relation between kidney function, proteinuria, and adverse outcomes. JAMA. 2010;303(5):423–429. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
