

Pathological Investigation of Congenital Bicuspid Aortic Valve Stenosis, Compared with Atherosclerotic Tricuspid Aortic Valve Stenosis and Congenital Bicuspid Aortic Valve Regurgitation
- PMID: 27479126
- PMCID: PMC4968844
- DOI: 10.1371/journal.pone.0160208
Pathological Investigation of Congenital Bicuspid Aortic Valve Stenosis, Compared with Atherosclerotic Tricuspid Aortic Valve Stenosis and Congenital Bicuspid Aortic Valve Regurgitation
Abstract
Background: Congenital bicuspid aortic valve (CBAV) is the main cause of aortic stenosis (AS) in young adults. However, the histopathological features of AS in patients with CBAV have not been fully investigated.
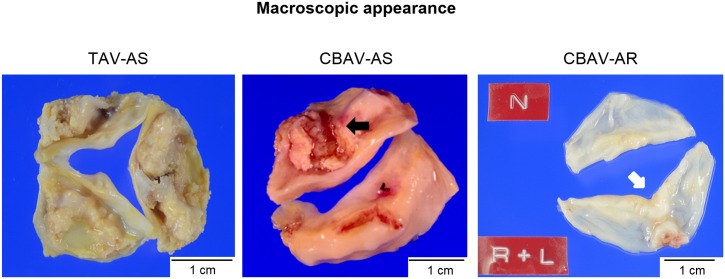
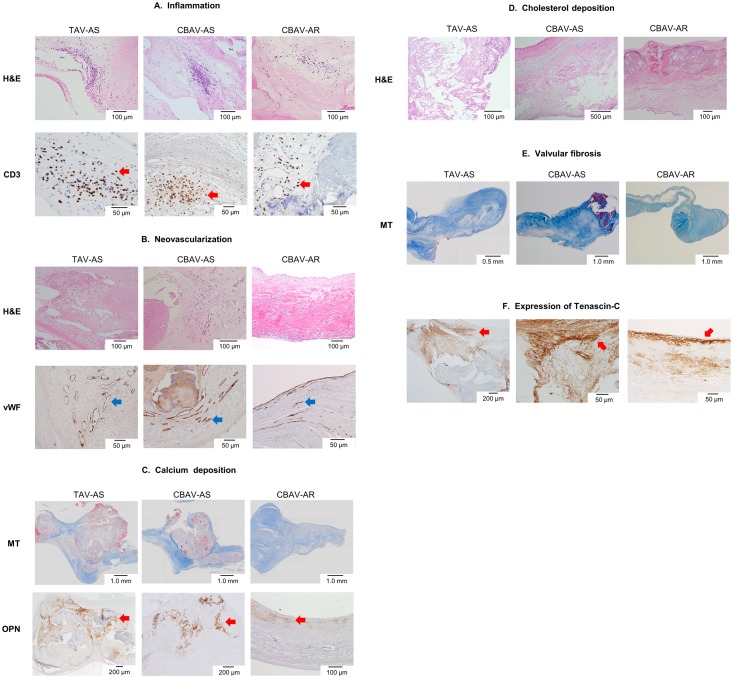
Methods and results: We examined specimens of aortic valve leaflets obtained from patients who had undergone aortic valve re/placement at our institution for severe AS with CBAV (n = 24, CBAV-AS group), severe AS with tricuspid aortic valve (n = 24, TAV-AS group), and severe aortic regurgitation (AR) with CBAV (n = 24, CBAV-AR group). We compared the histopathological features among the three groups. Pathological features were classified using semi-quantitative methods (graded on a scale 0 to 3) by experienced pathologists without knowledge of the patients' backgrounds. The severity of inflammation, neovascularization, and calcium and cholesterol deposition did not differ between the CBAV-AS and TAV-AS groups, and these four parameters were less marked in the CBAV-AR group than in the CBAV-AS (all p<0.01). Meanwhile, the grade of valvular fibrosis was greater in the CBAV-AS group, compared with the TAV-AS and CBAV-AR groups (both p<0.01). In AS patients, thickness of fibrotic lesions was greater on the aortic side than on the ventricular side (both p<0.01). Meanwhile, thickness of fibrotic lesions was comparable between the aortic and ventricular sides in CBAV-AR patients (p = 0.35).
Conclusions: Valvular fibrosis, especially on the aortic side, was greater in patients with CBAV-AS than in those without, suggesting a difference in the pathogenesis of AS between CBAV and TAV.
Conflict of interest statement
Figures
References
-
- Goldbarg SH, Elmariah S, Miller MA, Fuster V. Insights into degenerative aortic valve disease. J Am Coll Cardiol. 2007. September 25;50(13):1205–13. - PubMed
-
- Mohler ER 3rd, Gannon F, Reynolds C, Zimmerman R, Keane MG, Kaplan FS. Bone formation and inflammation in cardiac valves. Circulation. 2001. March 20;103(11):1522–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
