

Management of Invasive Differentiated Thyroid Cancer
- PMID: 27480110
- PMCID: PMC5118958
- DOI: 10.1089/thy.2016.0064
Management of Invasive Differentiated Thyroid Cancer
Abstract
Background: Invasive disease is a poor prognostic factor for patients with differentiated thyroid cancer (DTC). Uncontrolled central neck disease is a common cause of distressing death for patients presenting in this manner. Advances in assessment and management of such cases have led to significant improvements in outcome for this patient group. This article reviews the patterns of invasion and a contemporary approach to investigation and treatment of patients with invasive DTC.
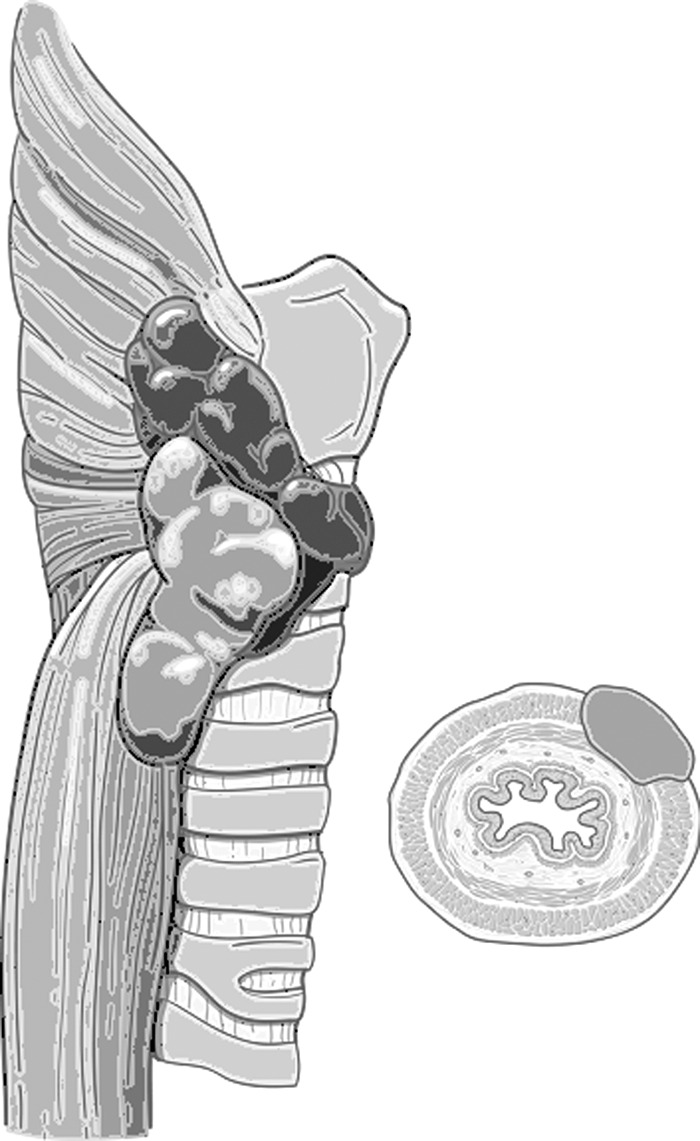
Summary: Aerodigestive tract invasion is reported in around 10% of case series of DTC. Assessment should include not only clinical history and physical examination with endoscopy as indicated, but ultrasound and contrast-enhanced cross-sectional imaging. Further studies including positron emission tomography should be considered, particularly in recurrent cases that are radioactive iodine (RAI) resistant. Both the patient and the extent of disease should be carefully assessed prior to embarking on surgery. The aim of surgery is to resect all gross disease. When minimal visceral invasion is encountered early, "shave" procedures are recommended. In the setting of transmural invasion of the airway or esophagus, however, full thickness excision is required. For intermediate cases in which invasion of the viscera has penetrated the superficial layers but is not evident in the submucosa, opinion is divided. Early reports recommended an aggressive approach. More recently authors have tended to recommend less aggressive resections with postoperative adjuvant therapies. The role of external beam radiotherapy continues to evolve in DTC with support for its use in patients considered to have RAI-resistant tumors.
Conclusions: Patients with invasive DTC require a multidisciplinary approach to investigation and treatment. With detailed assessment, appropriate surgery, and adjuvant therapy when indicated, this patient group can expect durable control of central neck disease, despite the aggressive nature of their primary tumors.
Conflict of interest statement
Author Disclosure Statement Dr. Kate Newbold has consultancy and advisory roles with Eisai, Astra-Zeneca, and Genzyme. The other authors have nothing to disclose.
Figures








References
-
- Davies L, Welch HG. 2006. Increasing incidence of thyroid cancer in the United States, 1973–2002. JAMA 295:2164–2167 - PubMed
-
- Hughes DT, Haymart MR, Miller BS, Gauger PG, Doherty GM. 2011. The most commonly occurring papillary thyroid cancer in the United States is now a microcarcinoma in a patient older than 45 years. Thyroid 21:231–236 - PubMed
-
- Nixon IJ, Ganly I, Patel SG, Palmer FL, Whitcher MM, Ghossein R, Tuttle MR, Shaha AR, Shah JP. 2012. Changing trends in well differentiated thyroid carcinoma over eight decades. Int J Surg 10:618–623 - PubMed
-
- Hay ID, Thompson GB, Grant CS, Bergstralh EJ, Dvorak CE, Gorman CA, Maurer MS, McIver B, Mullan BP, Oberg AL, Powell CC, van Heerden JA, Goellner JR. 2002. Papillary thyroid carcinoma managed at the Mayo Clinic during six decades (1940–1999): temporal trends in initial therapy and long-term outcome in 2444 consecutively treated patients. World J Surg 26:879–885 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
