

Technology-Enabled Remote Monitoring and Self-Management - Vision for Patient Empowerment Following Cardiac and Vascular Surgery: User Testing and Randomized Controlled Trial Protocol
- PMID: 27480247
- PMCID: PMC4999307
- DOI: 10.2196/resprot.5763
Technology-Enabled Remote Monitoring and Self-Management - Vision for Patient Empowerment Following Cardiac and Vascular Surgery: User Testing and Randomized Controlled Trial Protocol
Abstract
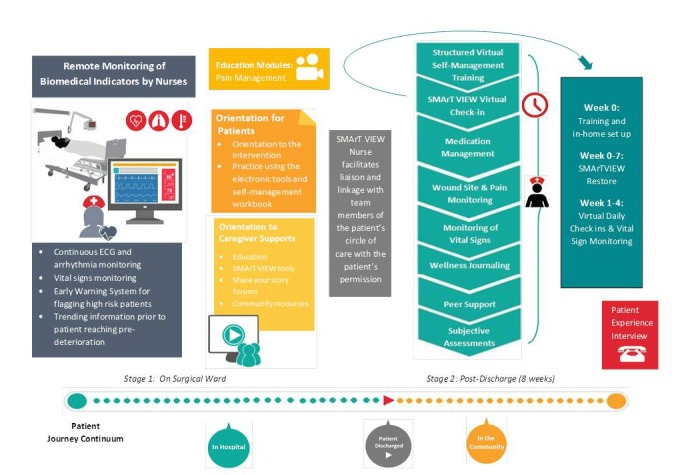
Background: Tens of thousands of cardiac and vascular surgeries (CaVS) are performed on seniors in Canada and the United Kingdom each year to improve survival, relieve disease symptoms, and improve health-related quality of life (HRQL). However, chronic postsurgical pain (CPSP), undetected or delayed detection of hemodynamic compromise, complications, and related poor functional status are major problems for substantial numbers of patients during the recovery process. To tackle this problem, we aim to refine and test the effectiveness of an eHealth-enabled service delivery intervention, TecHnology-Enabled remote monitoring and Self-MAnagemenT-VIsion for patient EmpoWerment following Cardiac and VasculaR surgery (THE SMArTVIEW, CoVeRed), which combines remote monitoring, education, and self-management training to optimize recovery outcomes and experience of seniors undergoing CaVS in Canada and the United Kingdom.
Objective: Our objectives are to (1) refine SMArTVIEW via high-fidelity user testing and (2) examine the effectiveness of SMArTVIEW via a randomized controlled trial (RCT).
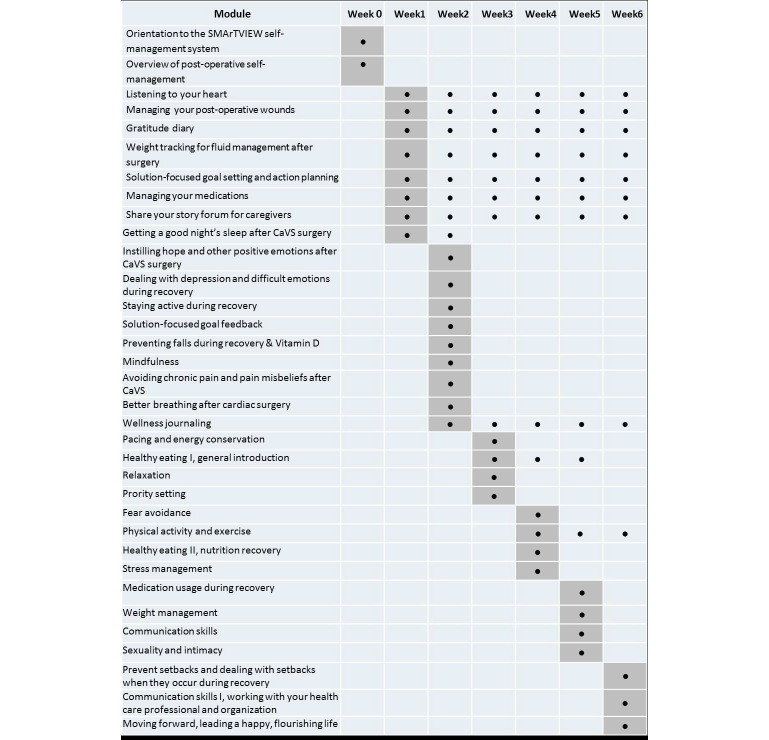
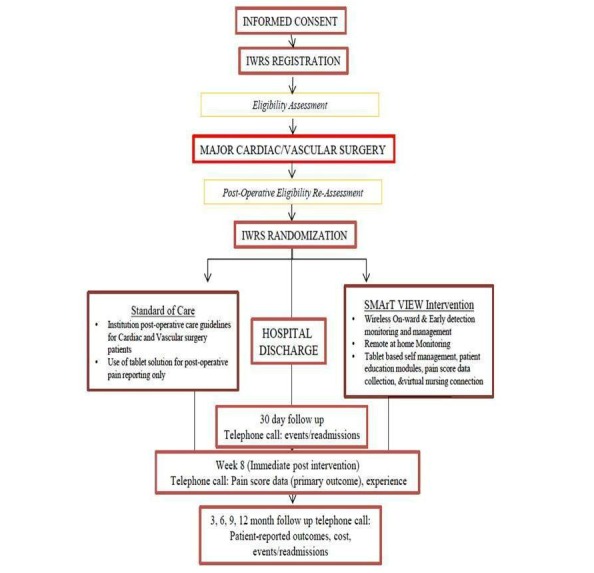
Methods: CaVS patients and clinicians will engage in two cycles of focus groups and usability testing at each site; feedback will be elicited about expectations and experience of SMArTVIEW, in context. The data will be used to refine the SMArTVIEW eHealth delivery program. Upon transfer to the surgical ward (ie, post-intensive care unit [ICU]), 256 CaVS patients will be reassessed postoperatively and randomly allocated via an interactive Web randomization system to the intervention group or usual care. The SMArTVIEW intervention will run from surgical ward day 2 until 8 weeks following surgery. Outcome assessments will occur on postoperative day 30; at week 8; and at 3, 6, 9, and 12 months. The primary outcome is worst postop pain intensity upon movement in the previous 24 hours (Brief Pain Inventory-Short Form), averaged across the previous 14 days. Secondary outcomes include a composite of postoperative complications related to hemodynamic compromise-death, myocardial infarction, and nonfatal stroke- all-cause mortality and surgical site infections, functional status (Medical Outcomes Study Short Form-12), depressive symptoms (Geriatric Depression Scale), health service utilization-related costs (health service utilization data from the Institute for Clinical Evaluative Sciences data repository), and patient-level cost of recovery (Ambulatory Home Care Record). A linear mixed model will be used to assess the effects of the intervention on the primary outcome, with an a priori contrast of weekly average worst pain intensity upon movement to evaluate the primary endpoint of pain at 8 weeks postoperation. We will also examine the incremental cost of the intervention compared to usual care using a regression model to estimate the difference in expected health care costs between groups.
Results: Study start-up is underway and usability testing is scheduled to begin in the fall of 2016.
Conclusions: Given our experience, dedicated industry partners, and related RCT infrastructure, we are confident we can make a lasting contribution to improving the care of seniors who undergo CaVS.
Keywords: randomized controlled trial; remote automated external monitoring; technology-enabled self-management; usability testing.
Conflict of interest statement
In-kind industry support is provided by the following industry partners: Philips, QoC Health, XAHIVE, and mPath. The following authors are employed by Philips: Karsten Russell Wood, Michael Weber, Jolene McNeil, and Robyn Alpert. Sarah Sharpe is Co-Founder and shareholder, QoC Health; Sue Bhella is employed by QoC Health. David Mohajer is Co-Founder, Chief Executive Officer, and Vice President, XAHIVE; Sem Ponnambalem is Co-Founder, Chief Operating Officer, and President, XAHIVE. Naeem Lakhani and Rabia Khan are Co-Founders, mPath.
Figures
Similar articles
-
Postoperative Remote Automated Monitoring and Virtual Hospital-to-Home Care System Following Cardiac and Major Vascular Surgery: User Testing Study.J Med Internet Res. 2020 Mar 18;22(3):e15548. doi: 10.2196/15548. J Med Internet Res. 2020. PMID: 32186521 Free PMC article.
-
Effectiveness and cost-effectiveness of a guided Internet- and mobile-based intervention for the indicated prevention of major depression in patients with chronic back pain-study protocol of the PROD-BP multicenter pragmatic RCT.BMC Psychiatry. 2017 Jan 21;17(1):36. doi: 10.1186/s12888-017-1193-6. BMC Psychiatry. 2017. PMID: 28109247 Free PMC article. Clinical Trial.
-
The effect of mobile app home monitoring on number of in-person visits following ambulatory surgery: protocol for a randomized controlled trial.JMIR Res Protoc. 2015 Jun 3;4(2):e65. doi: 10.2196/resprot.4352. JMIR Res Protoc. 2015. PMID: 26040252 Free PMC article.
-
Comparing Two Approaches to Help Patients Manage Symptoms at Home after Cancer Surgery — The ACCESS Study [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Nov. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Nov. PMID: 39432695 Free Books & Documents. Review.
-
Novel Augmentation Strategies in Major Depression.Dan Med J. 2017 Apr;64(4):B5338. Dan Med J. 2017. PMID: 28385173 Review.
Cited by
-
Electronic Health Interventions in the Case of Multiple Sclerosis: From Theory to Practice.Brain Sci. 2021 Feb 2;11(2):180. doi: 10.3390/brainsci11020180. Brain Sci. 2021. PMID: 33540640 Free PMC article. Review.
-
Systematic Review of Telemedicine and eHealth Systems Applied to Vascular Surgery.J Med Syst. 2022 Dec 6;46(12):104. doi: 10.1007/s10916-022-01895-z. J Med Syst. 2022. PMID: 36471095 Free PMC article.
-
Two-Way Social Media Messaging in Postoperative Cataract Surgical Patients: Prospective Interventional Study.J Med Internet Res. 2017 Dec 19;19(12):e413. doi: 10.2196/jmir.8330. J Med Internet Res. 2017. PMID: 29258973 Free PMC article.
-
The need for novel strategies to address postoperative pain associated with cardiac surgery: A commentary and introduction to "SMArTVIEW".Can J Pain. 2019 Jul 30;3(2):26-35. doi: 10.1080/24740527.2019.1603076. eCollection 2019. Can J Pain. 2019. PMID: 35005416 Free PMC article.
-
Emerging Role of Remote Patient Monitoring in Pulmonary Care: Telemedicine to Smart Phone.Chest. 2021 Feb;159(2):477-478. doi: 10.1016/j.chest.2020.10.015. Chest. 2021. PMID: 33563433 Free PMC article. No abstract available.
References
-
- McGillion M, Turner A, Carroll SL, Furze G, Busse J, Lamy A. Optimising self-management to reduce chronic pain and disability after cardiac surgery. Br J Cardiol. 2015;22:38. doi: 10.5837/bjc.2015.011. - DOI
-
- Gill NP, Wright B, Reilly CS. Relationship between hypoxaemic and cardiac ischaemic events in the perioperative period. Br J Anaesth. 1992 May;68(5):471–473. - PubMed
-
- Vascular Events In Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators. Devereaux PJ, Chan MT, Alonso-Coello P, Walsh M, Berwanger O, Villar JC, Wang CY, Garutti RI, Jacka MJ, Sigamani A, Srinathan S, Biccard BM, Chow CK, Abraham V, Tiboni M, Pettit S, Szczeklik W, Lurati BG, Botto F, Guyatt G, Heels-Ansdell D, Sessler DI, Thorlund K, Garg AX, Mrkobrada M, Thomas S, Rodseth RN, Pearse RM, Thabane L, McQueen MJ, VanHelder T, Bhandari M, Bosch J, Kurz A, Polanczyk C, Malaga G, Nagele P, Le MY, Leuwer M, Yusuf S. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA. 2012 Jun 6;307(21):2295–2304. doi: 10.1001/jama.2012.5502.1172044 - DOI - PubMed
-
- POISE Study Group. Devereaux PJ, Yang H, Yusuf S, Guyatt G, Leslie K, Villar JC, Xavier D, Chrolavicius S, Greenspan L, Pogue J, Pais P, Liu L, Xu S, Málaga G, Avezum A, Chan M, Montori VM, Jacka M, Choi P. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): A randomised controlled trial. Lancet. 2008 May 31;371(9627):1839–1847. doi: 10.1016/S0140-6736(08)60601-7. http://linkinghub.elsevier.com/retrieve/pii/S0140-6736(08)60601-7 S0140-6736(08)60601-7 - DOI - PubMed
-
- Devereaux PJ, Mrkobrada M, Sessler DI, Leslie K, Alonso-Coello P, Kurz A, Villar JC, Sigamani A, Biccard BM, Meyhoff CS, Parlow JL, Guyatt G, Robinson A, Garg AX, Rodseth RN, Botto F, Lurati BG, Xavier D, Chan MY, Tiboni M, Cook D, Kumar PA, Forget P, Malaga G, Fleischmann E, Amir M, Eikelboom J, Mizera R, Torres D, Wang CY, VanHelder T, Paniagua P, Berwanger O, Srinathan S, Graham M, Pasin L, Le Manach Y, Gao P, Pogue J, Whitlock R, Lamy A, Kearon C, Baigent C, Chow C, Pettit S, Chrolavicius S, Yusuf S, POISE-2 Investigators Aspirin in patients undergoing noncardiac surgery. N Engl J Med. 2014 Apr 17;370(16):1494–1503. doi: 10.1056/NEJMoa1401105. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
