

Effects of dexmedetomidine and esmolol on systemic hemodynamics and exogenous lactate clearance in early experimental septic shock
- PMID: 27480413
- PMCID: PMC4969982
- DOI: 10.1186/s13054-016-1419-x
Effects of dexmedetomidine and esmolol on systemic hemodynamics and exogenous lactate clearance in early experimental septic shock
Abstract
Background: Persistent hyperlactatemia during septic shock is multifactorial. Hypoperfusion-related anaerobic production and adrenergic-driven aerobic generation together with impaired lactate clearance have been implicated. An excessive adrenergic response could contribute to persistent hyperlactatemia and adrenergic modulation might be beneficial. We assessed the effects of dexmedetomidine and esmolol on hemodynamics, lactate generation, and exogenous lactate clearance during endotoxin-induced septic shock.
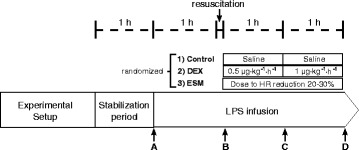
Methods: Eighteen anesthetized and mechanically ventilated sheep were subjected to a multimodal hemodynamic/perfusion assessment including hepatic and portal vein catheterizations, total hepatic blood flow, and muscle microdialysis. After monitoring, all received a bolus and continuous infusion of endotoxin. After 1 h they were volume resuscitated, and then randomized to endotoxin-control, endotoxin-dexmedetomidine (sequential doses of 0.5 and 1.0 μg/k/h) or endotoxin-esmolol (titrated to decrease basal heart rate by 20 %) groups. Samples were taken at four time points, and exogenous lactate clearance using an intravenous administration of sodium L-lactate (1 mmol/kg) was performed at the end of the experiments.
Results: Dexmedetomidine and esmolol were hemodynamically well tolerated. The dexmedetomidine group exhibited lower epinephrine levels, but no difference in muscle lactate. Despite progressive hypotension in all groups, both dexmedetomidine and esmolol were associated with lower arterial and portal vein lactate levels. Exogenous lactate clearance was significantly higher in the dexmedetomidine and esmolol groups.
Conclusions: Dexmedetomidine and esmolol were associated with lower arterial and portal lactate levels, and less impairment of exogenous lactate clearance in a model of septic shock. The use of dexmedetomidine and esmolol appears to be associated with beneficial effects on gut lactate generation and lactate clearance and exhibits no negative impact on systemic hemodynamics.
Keywords: Dexmedetomidine; Esmolol; Lactate; Lactate clearance; Septic shock.
Figures

Similar articles
-
Impairment of exogenous lactate clearance in experimental hyperdynamic septic shock is not related to total liver hypoperfusion.Crit Care. 2015 Apr 22;19(1):188. doi: 10.1186/s13054-015-0928-3. Crit Care. 2015. PMID: 25898244 Free PMC article.
-
Hemodynamic and anti-inflammatory effects of early esmolol use in hyperkinetic septic shock: a pilot study.Crit Care. 2021 Jan 7;25(1):21. doi: 10.1186/s13054-020-03445-w. Crit Care. 2021. PMID: 33413583 Free PMC article.
-
[Esmolol improves clinical outcome and tissue oxygen metabolism in patients with septic shock through controlling heart rate].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015 Sep;27(9):759-63. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2015. PMID: 26955704 Clinical Trial. Chinese.
-
Esmolol. A review of its therapeutic efficacy and pharmacokinetic characteristics.Clin Pharmacokinet. 1995 Mar;28(3):190-202. doi: 10.2165/00003088-199528030-00002. Clin Pharmacokinet. 1995. PMID: 7758250 Review.
-
Misdirected Sympathy: The Role of Sympatholysis in Sepsis and Septic Shock.J Intensive Care Med. 2018 Feb;33(2):74-86. doi: 10.1177/0885066616689548. Epub 2017 Jan 31. J Intensive Care Med. 2018. PMID: 28142307 Review.
Cited by
-
The influence of esmolol on right ventricular function in early experimental endotoxic shock.Physiol Rep. 2018 Sep;6(19):e13882. doi: 10.14814/phy2.13882. Physiol Rep. 2018. PMID: 30318855 Free PMC article.
-
Brain protective effect and hemodynamics of dexmedetomidine hydrochloride in patients with intracranial aneurysm.Saudi J Biol Sci. 2020 Jul;27(7):1850-1855. doi: 10.1016/j.sjbs.2020.03.027. Epub 2020 Apr 10. Saudi J Biol Sci. 2020. PMID: 33209088 Free PMC article.
-
The influence of metoprolol in patients with sepsis-induced cardiomyopathy: A retrospective study.Saudi Med J. 2023 Oct;44(10):1030-1036. doi: 10.15537/smj.2023.44.10.20230149. Saudi Med J. 2023. PMID: 37777259 Free PMC article.
-
Dexmedetomidine Has Differential Effects on the Contractility of Equine Jejunal Smooth Muscle Layers In Vitro.Animals (Basel). 2023 Mar 10;13(6):1021. doi: 10.3390/ani13061021. Animals (Basel). 2023. PMID: 36978562 Free PMC article.
-
[Changes in blood oxygen metabolism indices and their clinical significance in children with septic shock].Zhongguo Dang Dai Er Ke Za Zhi. 2017 Oct;19(10):1124-1128. doi: 10.7499/j.issn.1008-8830.2017.10.018. Zhongguo Dang Dai Er Ke Za Zhi. 2017. PMID: 29046213 Free PMC article. Chinese.
References
-
- Hernandez G, Castro R, Romero C, de la Hoz C, Angulo D, Aranguiz I, et al. Persistent sepsis-induced hypotension without hyperlactatemia: is it really septic shock? J Crit Care. 2011;435:e9–14. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
