

Contact Lens-induced Limbal Stem Cell Deficiency
- PMID: 27480488
- PMCID: PMC5065783
- DOI: 10.1016/j.jtos.2016.06.003
Contact Lens-induced Limbal Stem Cell Deficiency
Abstract
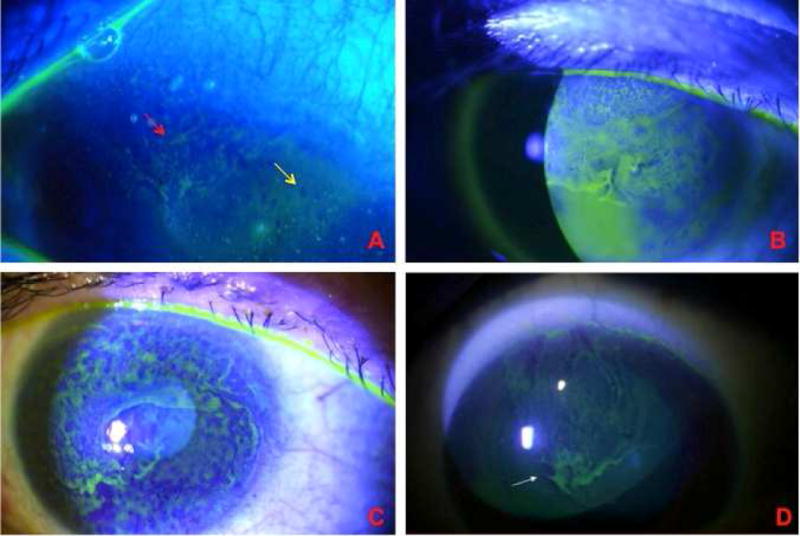
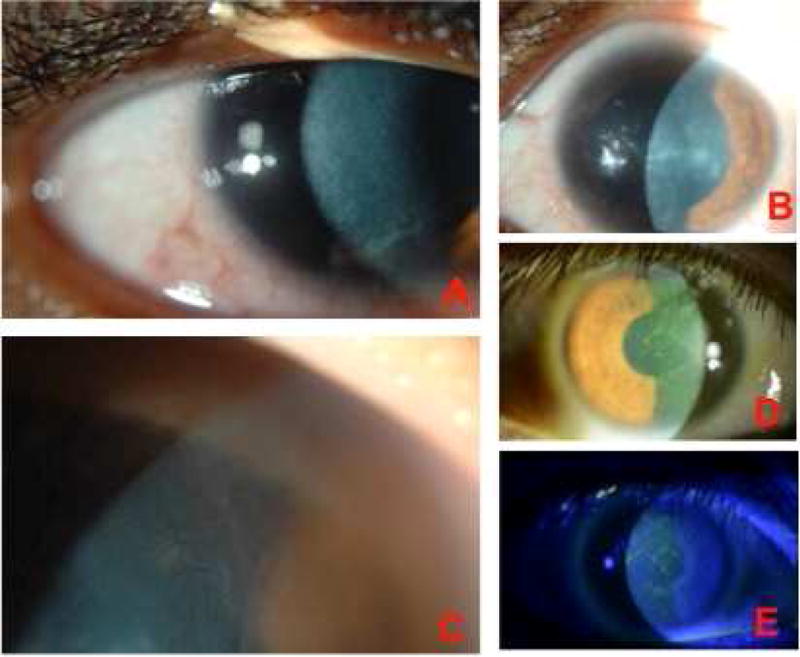
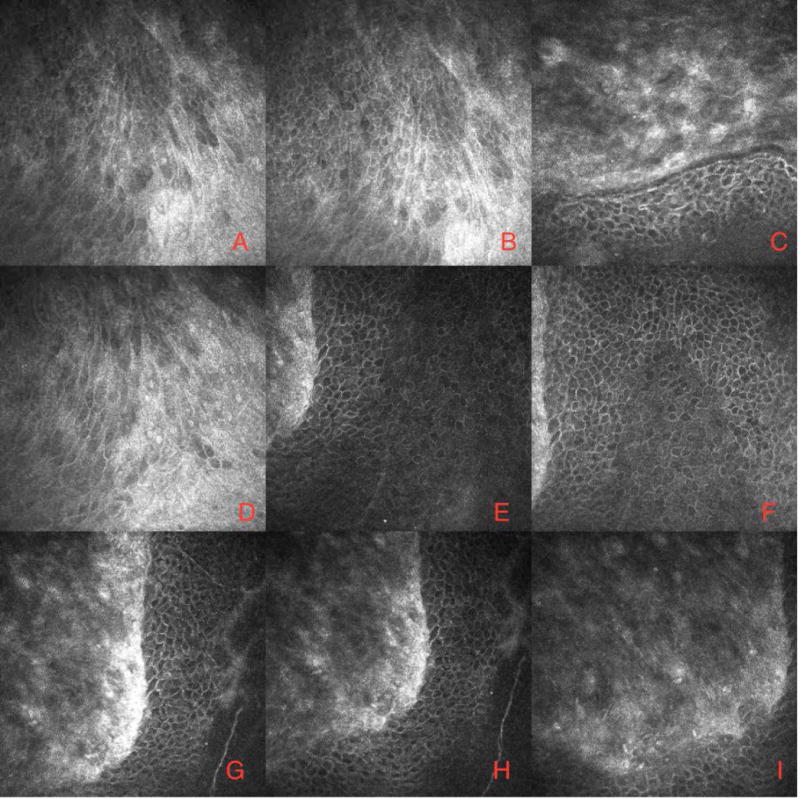
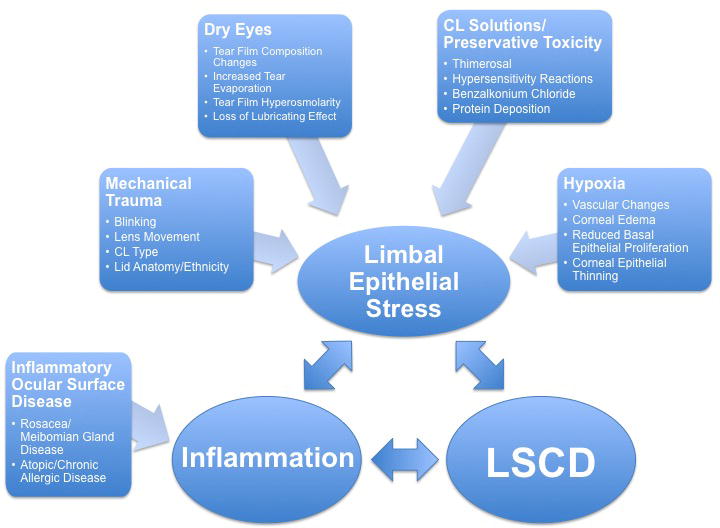
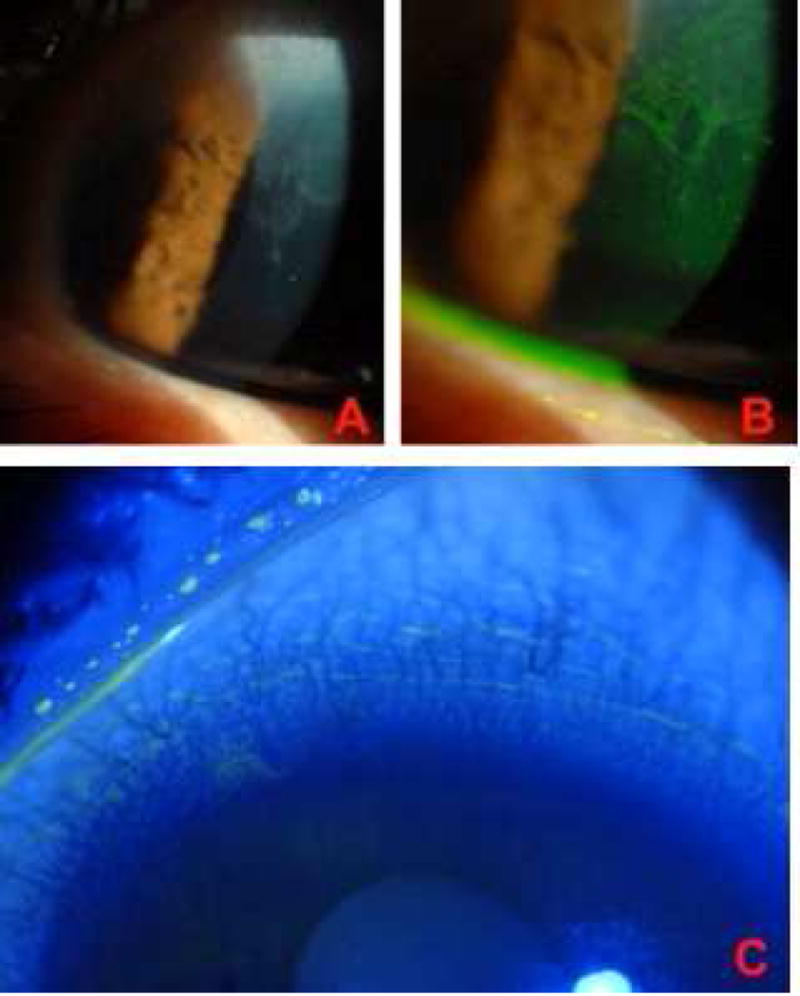
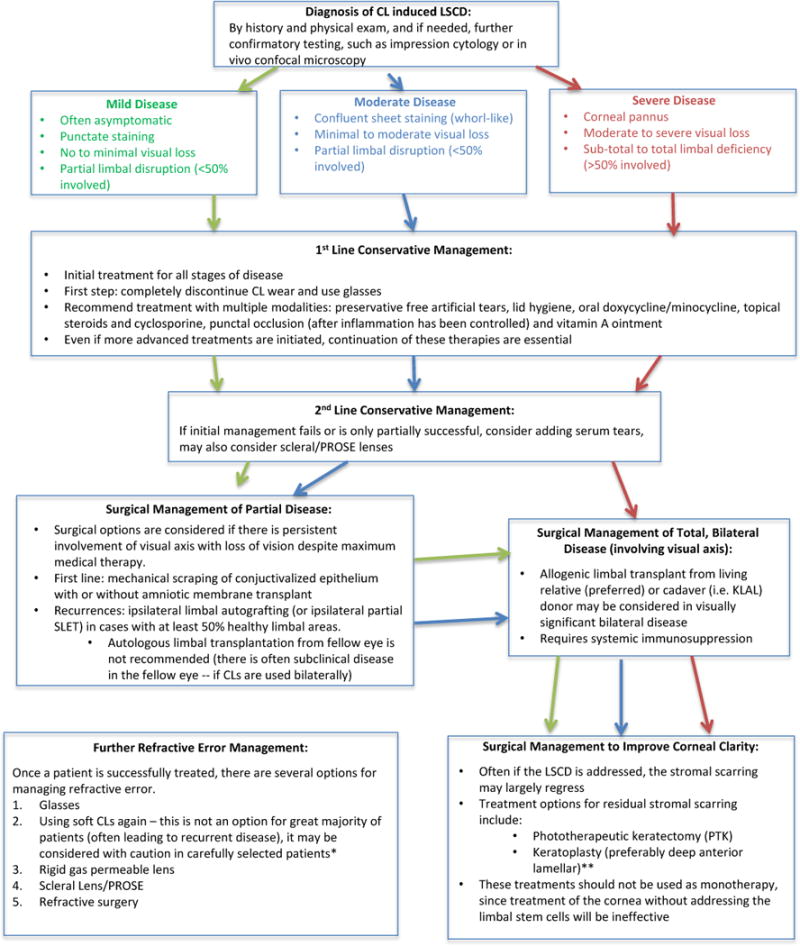
Limbal stem cell deficiency (LSCD) is a pathologic condition caused by the dysfunction and/or destruction of stem cell precursors of the corneal epithelium, typified clinically by corneal conjunctivalization. The purpose of this review is to critically discuss a less well-known cause of limbal stem cell disease: contact lens (CL) wear. A literature search was conducted to include original articles containing patients with CL-induced LSCD. This review describes epidemiology, diagnostic strategies, pathogenesis, differential diagnosis, and treatment modalities for this condition.
Keywords: contact lens; corneal conjunctivalization; limbal stem cell deficiency; limbal stem cells.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no commercial or proprietary interest in any concept or product discussed in this article.
Figures
Similar articles
-
Severe limbal stem cell deficiency from contact lens wear: patient clinical features.Am J Ophthalmol. 2013 Mar;155(3):544-549.e2. doi: 10.1016/j.ajo.2012.09.013. Epub 2012 Dec 4. Am J Ophthalmol. 2013. PMID: 23218703
-
Contact Lens Induced Limbal Stem Cell Deficiency: Clinical Features in Korean Patients.Korean J Ophthalmol. 2019 Dec;33(6):500-505. doi: 10.3341/kjo.2019.0095. Korean J Ophthalmol. 2019. PMID: 31833246 Free PMC article.
-
Presentation, diagnosis and management of limbal stem cell deficiency.Middle East Afr J Ophthalmol. 2013 Jan-Mar;20(1):5-10. doi: 10.4103/0974-9233.106381. Middle East Afr J Ophthalmol. 2013. PMID: 23580847 Free PMC article. Review.
-
Plasma polymer-coated contact lenses for the culture and transfer of corneal epithelial cells in the treatment of limbal stem cell deficiency.Tissue Eng Part A. 2014 Feb;20(3-4):646-55. doi: 10.1089/ten.TEA.2013.0089. Epub 2014 Jan 23. Tissue Eng Part A. 2014. PMID: 24328453 Free PMC article.
-
The diagnosis of limbal stem cell deficiency.Ocul Surf. 2018 Jan;16(1):58-69. doi: 10.1016/j.jtos.2017.11.002. Epub 2017 Nov 4. Ocul Surf. 2018. PMID: 29113917 Free PMC article. Review.
Cited by
-
Profile of biological characterizations and clinical application of corneal stem/progenitor cells.World J Stem Cells. 2022 Nov 26;14(11):777-797. doi: 10.4252/wjsc.v14.i11.777. World J Stem Cells. 2022. PMID: 36483848 Free PMC article. Review.
-
Therapeutic Strategies for Restoring Perturbed Corneal Epithelial Homeostasis in Limbal Stem Cell Deficiency: Current Trends and Future Directions.Cells. 2022 Oct 16;11(20):3247. doi: 10.3390/cells11203247. Cells. 2022. PMID: 36291115 Free PMC article. Review.
-
Evaluation of Medically Reversible Limbal Stem Cell Deficiency.Turk J Ophthalmol. 2024 Oct 25;54(5):251-256. doi: 10.4274/tjo.galenos.2024.69705. Turk J Ophthalmol. 2024. PMID: 39463138 Free PMC article.
-
Current and Emerging Therapies for Limbal Stem Cell Deficiency.Stem Cells Transl Med. 2022 Mar 31;11(3):259-268. doi: 10.1093/stcltm/szab028. Stem Cells Transl Med. 2022. PMID: 35303110 Free PMC article.
-
Emerging Therapeutic Strategies for Limbal Stem Cell Deficiency.J Ophthalmol. 2018 Jun 27;2018:7894647. doi: 10.1155/2018/7894647. eCollection 2018. J Ophthalmol. 2018. PMID: 30050691 Free PMC article. Review.
References
-
- Utheim TP. Limbal epithelial cell therapy: past, present, and future. In: Wright B, Connon CJ, editors. Methods In Molecular Biology: Cornea Regenerative Medicine: Methods and Protocols. New York, NY: Humana Press; 2013. pp. 3–43. - PubMed
-
- Thoft RA, Friend J. The X, Y, Z hypothesis of corneal epithelial maintenance. Invest Ophthalmol Vis Sci. 1983;24:1442–3. - PubMed
-
- Kruse FE, Chen JJY, Tsai RJF, Tseng SCG. Conjunctival transdifferentiation is due to the incomplete removal of limbal basal epithelium. Invest Ophthalmol Vis Sci. 1990;31:1903–13. - PubMed
-
- Majo F, Rochat A, Nicolas M, et al. Oligopotent stem cells are distributed throughout the mammalian ocular surface. Nature. 2008;13(7219):456. 250–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
