

High-Cost Patients: Hot-Spotters Don't Explain the Half of It
- PMID: 27480529
- PMCID: PMC5215147
- DOI: 10.1007/s11606-016-3790-3
High-Cost Patients: Hot-Spotters Don't Explain the Half of It
Abstract
Background: Understanding resource utilization patterns among high-cost patients may inform cost reduction strategies.
Objective: To identify patterns of high-cost healthcare utilization and associated clinical diagnoses and to quantify the significance of hot-spotters among high-cost users.
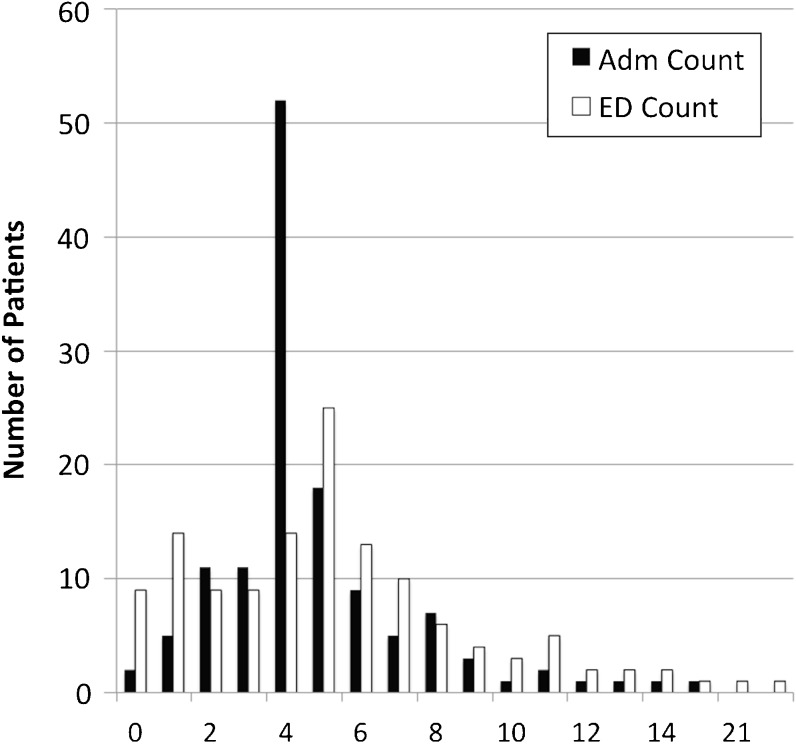
Design: Retrospective analysis of high-cost patients in 2012 using data from electronic medical records, internal cost accounting, and the Centers for Medicare and Medicaid Services. K-medoids cluster analysis was performed on utilization measures of the highest-cost decile of patients. Clusters were compared using clinical diagnoses. We defined "hot-spotters" as those in the highest-cost decile with ≥4 hospitalizations or ED visits during the study period.
Participants and exposure: A total of 14,855 Medicare Fee-for-service beneficiaries identified by the Medicare Quality Resource and Use Report as having received 100 % of inpatient care and ≥90 % of primary care services at Cleveland Clinic Health System (CCHS) in Northeast Ohio. The highest-cost decile was selected from this population.
Main measures: Healthcare utilization and diagnoses.
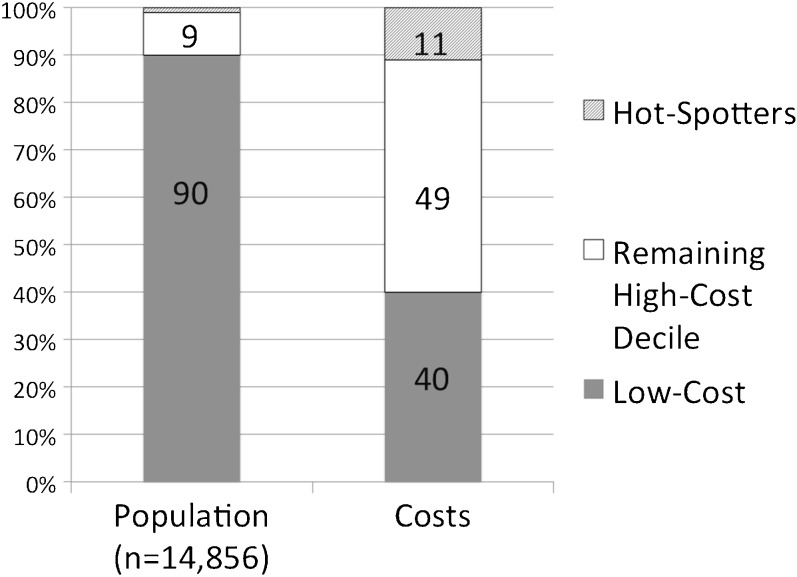
Key results: The highest-cost decile of patients (n = 1486) accounted for 60 % of total costs. We identified five patient clusters: "Ambulatory," with 0 admissions; "Surgical," with a median of 2 surgeries; "Critically Ill," with a median of 4 ICU days; "Frequent Care," with a median of 2 admissions, 3 ED visits, and 29 outpatient visits; and "Mixed Utilization," with 1 median admission and 1 ED visit. Cancer diagnoses were prevalent in the Ambulatory group, care complications in the Surgical group, cardiac diseases in the Critically Ill group, and psychiatric disorders in the Frequent Care group. Most hot-spotters (55 %) were in the "frequent care" cluster. Overall, hot-spotters represented 9 % of the high-cost population and accounted for 19 % of their overall costs.
Conclusions: High-cost patients are heterogeneous; most are not so-called "hot-spotters" with frequent admissions. Effective interventions to reduce costs will require a more multi-faceted approach to the high-cost population.
Keywords: High-cost; Hot-spotter.
Conflict of interest statement
Compliance with Ethical Standards Funders This study was conducted without funding. Prior Presentations Presented at the 38th Annual Society of General Internal Medicine National Meeting, Toronto, Canada, April 22, 2015. Conflicts of Interest There are no conflicts of interest to disclose.
Figures
Comment in
-
Hot-Spotters Aren't "The Problem"...But They Are Emblematic of the Failure of U.S. Healthcare.J Gen Intern Med. 2017 Jan;32(1):6-8. doi: 10.1007/s11606-016-3846-4. J Gen Intern Med. 2017. PMID: 27599488 Free PMC article. No abstract available.
-
Five High-Cost Patient Groups.J Gen Intern Med. 2017 Sep;32(9):965. doi: 10.1007/s11606-017-4105-z. J Gen Intern Med. 2017. PMID: 28653230 Free PMC article. No abstract available.
References
-
- Birnbaum H. A National Profile of Catastrophic Illness (NCHSR Research Summary Series). NCHSR Office of Scientific and Technical Information.
-
- Congressional Budget Office USC. Catastrophic Medical Expenses: Patterns in the Non-Elderly, Non-Poor Population. December 1982.
-
- Congressional Budget Office. High-Cost Medicare Beneficiaries. May 2005. http://www.cbo.gov/sites/default/files/cbofiles/ftpdocs/63xx/doc6332/05-.... Accessed June 2, 2016.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
