

Peak Plasma Concentration of Azithromycin and Treatment Responses in Mycobacterium avium Complex Lung Disease
- PMID: 27480854
- PMCID: PMC5038230
- DOI: 10.1128/AAC.00770-16
Peak Plasma Concentration of Azithromycin and Treatment Responses in Mycobacterium avium Complex Lung Disease
Abstract
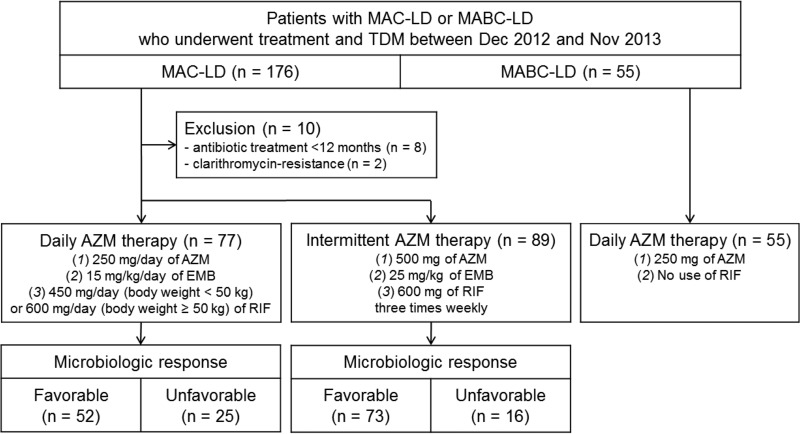
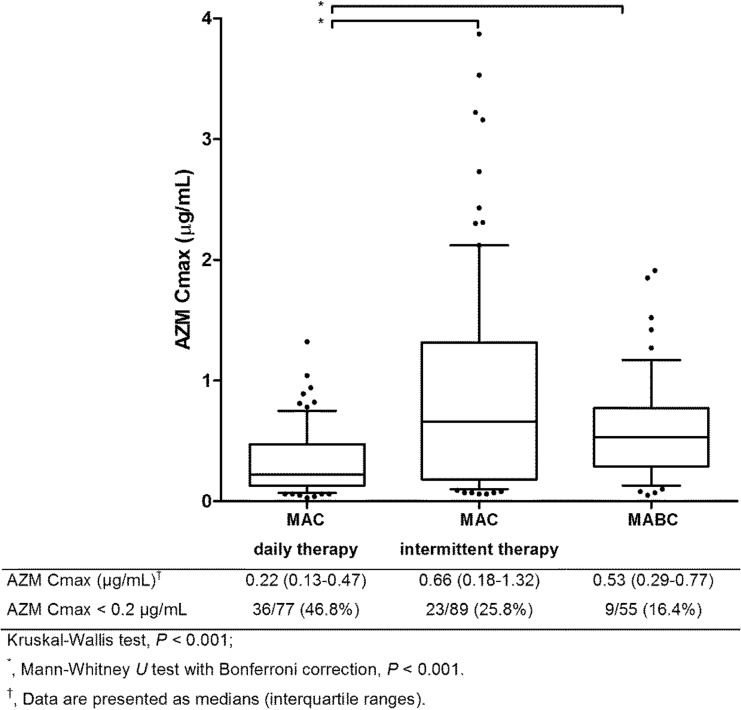
Macrolides, such as azithromycin (AZM) and clarithromycin, are the cornerstones of treatment for Mycobacterium avium complex lung disease (MAC-LD). Current guidelines recommend daily therapy with AZM for cavitary MAC-LD and intermittent therapy for noncavitary MAC-LD, but the effectiveness of these regimens has not been thoroughly investigated. This study evaluated associations between microbiological response and estimated peak plasma concentrations (Cmax) of AZM. The AZM Cmax was measured in patients receiving daily therapy (250 mg of AZM daily, n = 77) or intermittent therapy (500 mg of AZM three times weekly, n = 89) for MAC-LD and daily therapy for Mycobacterium abscessus complex LD (MABC-LD) (250 mg of AZM daily, n = 55). The AZM Cmax was lower with the daily regimen for MAC-LD (median, 0.24 μg/ml) than with the intermittent regimen for MAC-LD (median, 0.65 μg/ml; P < 0.001) or daily therapy for MABC-LD (median, 0.53 μg/ml; P < 0.001). After adjusting for confounding factors, AZM Cmax was independently associated with favorable microbiological responses in MAC-LD patients receiving a daily regimen (adjusted odds ratio [aOR], 1.58; 95% confidence interval [CI], 1.01 to 2.48; P = 0.044) but not an intermittent regimen (aOR, 0.85; 95% CI, 0.58 to 1.23, P = 0.379). With the daily AZM-based multidrug regimen for MAC-LD, a low AZM Cmax was common, whereas a higher AZM Cmax was associated with favorable microbiologic responses. The results also suggested that the addition of rifampin may lower AZM Cmax When a daily AZM-based multidrug regimen is used for treating severe MAC-LD, such as cavitary disease, the currently recommended AZM dose might be suboptimal. (This study has been registered at ClinicalTrials.gov under identifier NCT00970801.).
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures
Similar articles
-
Intermittent antibiotic therapy for nodular bronchiectatic Mycobacterium avium complex lung disease.Am J Respir Crit Care Med. 2015 Jan 1;191(1):96-103. doi: 10.1164/rccm.201408-1545OC. Am J Respir Crit Care Med. 2015. PMID: 25393520 Clinical Trial.
-
Analysis of drug treatment outcome in clarithromycin-resistant Mycobacterium avium complex lung disease.BMC Infect Dis. 2016 Jan 27;16:31. doi: 10.1186/s12879-016-1384-7. BMC Infect Dis. 2016. PMID: 26818764 Free PMC article.
-
Therapeutic drug monitoring in the treatment of Mycobacterium avium complex lung disease.Am J Respir Crit Care Med. 2012 Oct 15;186(8):797-802. doi: 10.1164/rccm.201206-1088OC. Epub 2012 Aug 9. Am J Respir Crit Care Med. 2012. PMID: 22878282
-
Treatment for Mycobacterium avium complex lung disease.J Formos Med Assoc. 2020 Jun;119 Suppl 1:S67-S75. doi: 10.1016/j.jfma.2020.05.006. Epub 2020 May 20. J Formos Med Assoc. 2020. PMID: 32446754 Review.
-
Risk-benefit assessment of therapies for Mycobacterium avium complex infections.Drug Saf. 1999 Aug;21(2):137-52. doi: 10.2165/00002018-199921020-00006. Drug Saf. 1999. PMID: 10456381 Review.
Cited by
-
Clinical pharmacists' interventions and therapeutic drug monitoring in patients with mycobacterial infections.J Clin Tuberc Other Mycobact Dis. 2023 Jan 13;30:100346. doi: 10.1016/j.jctube.2023.100346. eCollection 2023 Feb. J Clin Tuberc Other Mycobact Dis. 2023. PMID: 36683594 Free PMC article.
-
Case Commentary: A herculean effort for Mycobacterium heraklionense-localized azithromycin bead pharmacokinetics.Antimicrob Agents Chemother. 2025 Jun 4;69(6):e0030525. doi: 10.1128/aac.00305-25. Epub 2025 Apr 23. Antimicrob Agents Chemother. 2025. PMID: 40464553 Free PMC article.
-
Minimum inhibitory concentrations of azithromycin in clinical isolates of Mycobacterium avium complex in Japan.Microbiol Spectr. 2024 Jun 4;12(6):e0021824. doi: 10.1128/spectrum.00218-24. Epub 2024 Apr 30. Microbiol Spectr. 2024. PMID: 38687080 Free PMC article.
-
Intermittent Treatment with Azithromycin and Ethambutol for Noncavitary Mycobacterium avium Complex Pulmonary Disease.Antimicrob Agents Chemother. 2019 Dec 20;64(1):e01787-19. doi: 10.1128/AAC.01787-19. Print 2019 Dec 20. Antimicrob Agents Chemother. 2019. PMID: 31611366 Free PMC article.
-
An Overview of Various Rifampicin Analogs against Mycobacterium tuberculosis and their Drug Interactions.Med Chem. 2024;20(3):268-292. doi: 10.2174/0115734064260853230926080134. Med Chem. 2024. PMID: 37855280 Review.
References
-
- Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, Holland SM, Horsburgh R, Huitt G, Iademarco MF, Iseman M, Olivier K, Ruoss S, von Reyn CF, Wallace RJ Jr, Winthrop K, ATS Mycobacterial Diseases Subcommittee, American Thoracic Society, Infectious Diseases Society of America. 2007. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 175:367–416. doi:10.1164/rccm.200604-571ST. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
